Cavernous sinus thrombosis
| Cavernous sinus thrombosis | |
|---|---|
|
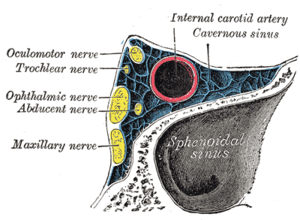
Oblique section through the cavernous sinus. | |
| Classification and external resources | |
| Specialty | neurology |
| ICD-10 | G08 |
| ICD-9-CM | 325 |
| DiseasesDB | 2184 |
| MedlinePlus | 001628 |
| eMedicine | emerg/87 neuro/572 |
| MeSH | D020226 |
Cavernous sinus thrombosis (CST) is the formation of a blood clot within the cavernous sinus, a cavity at the base of the brain which drains deoxygenated blood from the brain back to the heart. The cause is usually from a spreading infection in the nose, sinuses, ears, or teeth. Staphylococcus aureus and Streptococcus are often the associated bacteria. Cavernous sinus thrombosis symptoms include: decrease or loss of vision, chemosis, exophthalmos (bulging eyes), headaches, and paralysis of the cranial nerves which course through the cavernous sinus. This infection is life-threatening and requires immediate treatment, which usually includes antibiotics and sometimes surgical drainage.[1]
Clinical features
The clinical presentation of CST can be varied. Both acute, fulminant disease and indolent, subacute presentations have been reported in the literature.
The most common signs of CST are related to anatomical structures affected within the cavernous sinus, notably cranial nerves III-VI, as well as symptoms resulting from impaired venous drainage from the orbit and eye.
Classic presentations are abrupt onset of unilateral periorbital edema, headache, photophobia, and bulging of the eye (proptosis).[2]
Other common signs and symptoms include:
Ptosis, chemosis, cranial nerve palsies (III, IV, V, VI). Sixth nerve palsy is the most common. Sensory deficits of the ophthalmic and maxillary branch of the fifth nerve are common. Periorbital sensory loss and impaired corneal reflex may be noted. Papilledema, retinal hemorrhages, and decreased visual acuity and blindness may occur from venous congestion within the retina. Fever, tachycardia and sepsis may be present. Headache with nuchal rigidity may occur. Pupil may be dilated and sluggishly reactive. Infection can spread to contralateral cavernous sinus within 24–48 hours of initial presentation.[2]
Etiology
CST most commonly results from contiguous spread of infection from a nasal furuncle (50%), sphenoidal or ethmoidal sinuses (30%) and dental infections (10%).[3] Less common primary sites of infection include tonsils, soft palate, middle ear, or orbit (orbital cellulitis). The highly anastomotic venous system of the paranasal sinuses allows retrograde spread of infection to the cavernous sinus via the superior and inferior ophthalmic veins. It was previously thought that veins in the area were valveless and that this was the major cause of the retrograde spread, however, a recent study has found that the ophthalmic and facial veins are not valveless.[4]
Staphylococcus aureus is the most common infectious microbe, found in 70% of the cases.[3] Streptococcus is the second leading cause. Gram-negative rods and anaerobes may also lead to cavernous sinus thrombosis. Rarely, Aspergillus fumigatus and mucormycosis cause CST.
Diagnosis
The diagnosis of cavernous sinus thrombosis is made clinically, with imaging studies to confirm the clinical impression. Proptosis, ptosis, chemosis, and cranial nerve palsy beginning in one eye and progressing to the other eye establish the diagnosis.
Differential diagnosis
- Orbital cellulitis
- Internal carotid artery aneurysm
- Stroke
- Migraine headache
- Allergic blepharitis
- Thyroid exophthalmos
- Brain tumor
- Meningitis
- Mucormycosis
- Trauma
Workup
Cavernous sinus thrombosis is a clinical diagnosis with laboratory tests and imaging studies confirming the clinical impression.
Laboratory tests
CBC, ESR, blood cultures, and sinus cultures help establish and identify an infectious primary source. Lumbar puncture is necessary to rule out meningitis.
Imaging studies
Sinus films are helpful in the diagnosis of sphenoid sinusitis. Opacification, sclerosis, and air-fluid levels are typical findings. Contrast-enhanced CT scan may reveal underlying sinusitis, thickening of the superior ophthalmic vein, and irregular filling defects within the cavernous sinus; however, findings may be normal early in the disease course.
A MRI using flow parameters and an MR venogram are more sensitive than a CT scan, and are the imaging studies of choice to diagnose cavernous sinus thrombosis. Findings may include deformity of the internal carotid artery within the cavernous sinus, and an obvious signal hyperintensity within thrombosed vascular sinuses on all pulse sequences.
Cerebral angiography can be performed, but it is invasive and not very sensitive. Orbital venography is difficult to perform, but it is excellent in diagnosing occlusion of the cavernous sinus.
Treatment
According to the ICD-9M code, cavernous sinus thrombosis has a mortality rate of less than 20% in areas with access to antibiotics. Before antibiotics were available, the mortality was 80–100%. Morbidity rates also dropped from 70% to 22% due to earlier diagnosis and treatment.
Non-pharmacologic therapy
Recognizing the primary source of infection (i.e., facial cellulitis, middle ear, and sinus infections) and treating the primary source expeditiously is the best way to prevent cavernous sinus thrombosis.
Acute general treatment
Broad-spectrum intravenous antibiotics are used until a definite pathogen is found.
- Nafcillin 1.5 g IV q4h
- Cefotaxime 1.5 to 2 g IV q4h
- Metronidazole 15 mg/kg load followed by 7.5 mg/kg IV q6h
Vancomycin may be substituted for nafcillin if significant concern exists for infection by methicillin-resistant Staphylococcus aureus or resistant Streptococcus pneumoniae.[5] Appropriate therapy should take into account the primary source of infection as well as possible associated complications such as brain abscess, meningitis, or subdural empyema.
Anticoagulation with heparin is controversial. Retrospective studies show conflicting data. This decision should be made with subspecialty consultation.[6] One systematic review concluded that anticoagulation treatment appeared safe and was associated with a potentially important reduction in the risk of death or dependency.[7]
Steroid therapy is also controversial in many cases of CST.[8][9][10][11] However, corticosteroids are absolutely indicated in cases of pituitary insufficiency. Corticosteroid use may have a critical role in patients with Addisonian crisis secondary to ischaemia or necrosis of the pituitary that complicates CST.[12][13]
Long-term treatment
Surgical drainage with sphenoidotomy is indicated if the primary site of infection is thought to be the sphenoidal sinuses.
All patients with CST are usually treated with prolonged courses (3–4 weeks) of IV antibiotics. If there is evidence of complications such as intracranial suppuration, 6–8 weeks of total therapy may be warranted.
All patients should be monitored for signs of complicated infection, continued sepsis, or septic emboli while antibiotic therapy is being administered.
Key points
Cavernous sinus thrombosis can be a life-threatening, rapidly progressive infectious disease with high morbidity and mortality rates despite antibiotic use.
Complications of untreated CST include extension of thrombus to other dural venous sinuses, carotid thrombosis with concomitant strokes, subdural empyema, brain abscess, or meningitis. Septic embolization may also occur to the lungs, resulting in acute respiratory distress syndrome, pulmonary abscess, empyema, and pneumothorax.
Complications in treated patients include oculomotor weakness, blindness, pituitary insufficiency, and hemiparesis.
References
- ↑ "Cavernous sinus thrombosis - NHS Choices". www.nhs.uk. NHS Choices. Retrieved 27 May 2016.
- 1 2 "Cavernous sinus thrombosis: MedlinePlus Medical Encyclopedia". www.nlm.nih.gov. Retrieved 27 May 2016.
- 1 2 http://www.merckmanuals.com/professional/sec09/ch108/ch108b.html
- ↑ Zhang J, Stringer MD (July 2010). "Ophthalmic and facial veins are not valveless". Clin. Experiment. Ophthalmol. 38 (5): 502–10. doi:10.1111/j.1442-9071.2010.02325.x. PMID 20491800.
- ↑ Munckhof WJ, Krishnan A, Kruger P, Looke D (April 2008). "Cavernous sinus thrombosis and meningitis from community-acquired methicillin-resistant Staphylococcus aureus infection". Intern Med J. 38 (4): 283–7. doi:10.1111/j.1445-5994.2008.01650.x. PMID 18380704.
- ↑ Bhatia, K; Jones, NS (September 2002). "Septic cavernous sinus thrombosis secondary to sinusitis: are anticoagulants indicated? A review of the literature.". The Journal of laryngology and otology. 116 (9): 667–76. doi:10.1258/002221502760237920. PMID 12437798.
- ↑ Coutinho, J; de Bruijn, SF; Deveber, G; Stam, J (2011). "Anticoagulation for cerebral sinus thrombosis". Cochrane Database Syst Rev. (CD002005). doi:10.1002/14651858.cd002005.pub2.
- ↑ Southwick, FS; Richardson EP, Jr; Swartz, MN (March 1986). "Septic thrombosis of the dural venous sinuses.". Medicine. 65 (2): 82–106. doi:10.1097/00005792-198603000-00002. PMID 3512953.
- ↑ Gallagher, RM; Gross, CW; Phillips, CD (November 1998). "Suppurative intracranial complications of sinusitis.". The Laryngoscope. 108 (11 Pt 1): 1635–42. doi:10.1097/00005537-199811000-00009. PMID 9818818.
- ↑ Clifford-Jones, RE; Ellis, CJ; Stevens, JM; Turner, A (1 December 1982). "Cavernous sinus thrombosis.". Journal of Neurology, Neurosurgery & Psychiatry. 45 (12): 1092–1097. doi:10.1136/jnnp.45.12.1092.
- ↑ Igarashi, H; Igarashi, S; Fujio, N; Fukui, K; Yoshida, A (1995). "Magnetic resonance imaging in the early diagnosis of cavernous sinus thrombosis.". Ophthalmologica. Journal international d'ophtalmologie. International journal of ophthalmology. Zeitschrift fur Augenheilkunde. 209 (5): 292–6. doi:10.1159/000310635. PMID 8570157.
- ↑ Silver, HS; Morris, LR (May 1983). "Hypopituitarism Secondary to Cavernous Sinus Thrombosis". Southern Medical Journal. 76 (5): 642–646. doi:10.1097/00007611-198305000-00027.
- ↑ Sahjpaul, RL; Lee, DH (April 1999). "Infratentorial subdural empyema, pituitary abscess, and septic cavernous sinus thrombophlebitis secondary to paranasal sinusitis: case report.". Neurosurgery. 44 (4): 864–6; discussion 866–8. doi:10.1097/00006123-199904000-00101. PMID 10201313.
- Wald, ER (June 2007). "Periorbital and orbital infections.". Infectious disease clinics of North America. 21 (2): 393–408, vi. doi:10.1016/j.idc.2007.03.008. PMID 17561075.
- Osborn, Melissa K; Steinberg, James P (January 2007). "Subdural empyema and other suppurative complications of paranasal sinusitis". The Lancet Infectious Diseases. 7 (1): 62–67. doi:10.1016/S1473-3099(06)70688-0.