Prepatellar bursitis
| Prepatellar bursitis | |
|---|---|
| Synonyms | beat knee,[1] carpet layer's knee, coal miner's knee, housemaid's knee,[2] rug cutter's knee, nun's knee[3] |
 | |
| Aseptic prepatellar bursitis | |
| Classification and external resources | |
| Specialty | rheumatology |
| ICD-10 | M70.4 |
| ICD-9-CM | 726.65 |
| Patient UK | Prepatellar bursitis |
Prepatellar bursitis is an inflammation of the prepatellar bursa at the front of the knee. It is marked by swelling at the knee, which can be tender to the touch but which does not restrict the knee's range of motion. It is most commonly caused by trauma to the knee, either by a single acute instance or by chronic trauma over time. As such, prepatellar bursitis commonly occurs among individuals whose professions require frequent kneeling.
A definitive diagnosis of the condition can usually be made once a clinical history and physical examination have been obtained, though determining whether or not the bursitis is septic is not as straightforward. Treatment of prepatellar bursitis depends on the severity of the symptoms. Mild cases may only require rest and icing of the knee. A number of different treatment options have been used for severe septic cases, including intravenous antibiotics, surgical irrigation of the bursa, and bursectomy.
Signs and symptoms
The primary symptom of prepatellar bursitis is the swelling of the area around the kneecap. It generally does not produce a significant amount of pain unless pressure is applied directly to the swelling.[4] The area of swelling may be red (erythema), warm to the touch, or surrounded by cellulitis, particularly if the area has become infected. In such cases, the bursitis is often accompanied by fever.[5]:p. 608 Unlike arthritis, prepatellar bursitis generally does not affect the range of motion of the knee, though it may cause some discomfort when the knee is completely flexed.[6]:p. 360 Flexion and extension of the knee may cause crepitus.[7]:p. 20
Causes
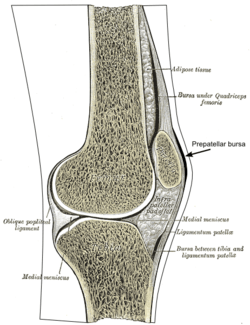
In human anatomy, a bursa is a small pouch filled with synovial fluid. Its purpose is to reduce friction between adjacent structures. The prepatellar bursa is one of several bursae of the knee joint, and is located between the patella and the skin.[8] Prepatellar bursitis is an inflammation of this bursa. Bursae are readily inflamed when irritated, as their walls are very thin.[7]:p. 22 Along with the pes anserine bursa, the prepatellar bursa is one of the most common bursae to cause knee pain when inflamed.[9]
Prepatellar bursitis is caused by either a single instance of acute trauma to the knee, or repeated minor trauma to the knee. The trauma can cause extravasation of nearby fluids into the bursa, which stimulates an inflammatory response.[2] This response occurs in two phases: The vascular phase, in which the blood flow to the surrounding area increases, and the cellular phase, in which leukocytes migrate from the blood to the affected area.[7]:p. 22 Other possible causes include gout, sarcoidosis, CREST syndrome,[6]:p. 359 diabetes mellitus, alcohol abuse, uremia, and chronic obstructive pulmonary disease.[7]:p. 22 Some cases are idiopathic, though these may be caused by trauma that the patient does not remember.[5]:pp. 607–8
The prepatellar bursa and the olecranon bursa are the two bursae that are most likely to become infected, or septic.[10] Septic bursitis typically occurs when the trauma to the knee causes an abrasion, though it is also possible for the infection to be caused by bacteria traveling through the blood from a pre-existing infection site.[11] In approximately 80% of septic cases, the infection is caused by Staphylococcus aureus; other common infections are Streptococcus, Mycobacterium, and Brucella.[6]:p. 359 It is highly unusual for septic bursitis to be caused by anaerobes, fungi, or Gram-negative bacteria.[5]:p. 608 In very rare cases, the infection can be caused by tuberculosis.[12]
Diagnosis
There are several types of inflammation that can cause knee pain, including sprains, bursitis, and injuries to the meniscus.[9] A diagnosis of prepatellar bursitis can be made based on a physical examination and the presence of risk factors in the person's medical history; swelling and tenderness at the front of the knee, combined with a profession that requires frequent kneeling, suggest prepatellar bursitis.[2] Swelling of multiple joints along with restricted range of motion may indicate arthritis instead.[5]:p. 608
A physical examination and medical history are generally not enough to distinguish between infectious and non-infectious bursitis; aspiration of the bursal fluid is often required for this, along with a cell culture and Gram stain of the aspirated fluid.[6]:p. 360 Septic prepatellar bursitis may be diagnosed if the fluid is found to have a neutrophil count above 1500 per microliter,[5]:p. 608 a threshold significantly lower than that of septic arthritis (50,000 cells per microliter).[6]:p. 360 A tuberculosis infection can be confirmed using a roentgenogram and urinalysis.[12]
Prevention
It is possible to prevent the onset of prepatellar bursitis, or prevent the symptoms from worsening, by avoiding trauma to the knee or frequent kneeling.[5]:p. 610 Protective knee pads can also help prevent prepatellar bursitis for those whose professions require frequent kneeling and for athletes who play contact sports, such as American football, basketball, and wrestling.[13]
Treatment
Non-septic prepatellar bursitis can be treated with rest, the application of ice to the affected area, and anti-inflammatory drugs, particularly ibuprofen. Elevation of the affected leg during rest may also expedite the recovery process.[13] Severe cases may require fine-needle aspiration of the bursa fluid, sometimes coupled with cortisone injections.[11] However, some studies have shown that steroid injections may not be an effective treatment option.[14] After the bursitis has been treated, rehabilitative exercise may help improve joint mechanics and reduce chronic pain.[15]:p. 2320
Opinions vary as to which treatment options are most effective for septic prepatellar bursitis.[6]:p. 360 McAfee and Smith recommend a course of oral antibiotics, usually oxacillin sodium or cephradine, and assert that surgery and drainage are unnecessary.[5]:p. 609 Wilson-MacDonald argues that oral antibiotics are "inadequate", and recommends intravenous antibiotics for managing the infection.[1] Some authors suggest surgical irrigation of the bursa by means of a subcutaneous tube.[6]:p. 360[16] Others suggest that bursectomy may be necessary for intractable cases; the operation is an outpatient procedure that can be performed in less than half an hour.[17]:p. 357
Epidemiology
The various nicknames associated with prepatellar bursitis arise from the fact that it commonly occurs among those individuals whose professions require frequent kneeling, such as carpenters, carpet layers, gardeners, housemaids, mechanics, miners, plumbers, and roofers.[2][4][5]:p. 607 The exact incidence of the condition is not known; it is difficult to estimate because only severe septic cases require hospital admission, and mild non-septic cases generally go unreported.[5]:p. 607 Prepatellar bursitis is more common among males than females. It affects all age groups, but is more likely to be septic when it occurs in children.[18]
References
- 1 2 Wilson-Macdonald, James (1987). "Management and outcome of infective prepatellar bursitis". Postgrad Med J. 63 (744): 851–853. doi:10.1136/pgmj.63.744.851. PMC 2428634
 . PMID 3447109.
. PMID 3447109. - 1 2 3 4 Madsen, James M (22 November 2004). "Prepatellar Bursitis". In Greenberg, Michael I. Greenberg's Text-Atlas of Emergency Medicine. Lippincott Williams & Wilkins. p. 922. ISBN 9780781745864.
- ↑ http://www.icd9data.com/2012/Volume1/710-739/725-729/727/727.2.htm
- 1 2 Biundo, Joseph J (2008). "Prepatellar Bursitis". In Klippel, John H. Primer on the Rheumatic Diseases. Springer. p. 80. ISBN 9780387356648.
- 1 2 3 4 5 6 7 8 9 McAfee, JH; Smith, DL (November 1988). "Olecranon and prepatellar bursitis—Diagnosis and treatment" (PDF). West J Med. 149 (5): 607–610. PMC 1026560. PMID 3074561.
- 1 2 3 4 5 6 7 Aaron, DL; et al. (June 2011). "Four common types of bursitis: diagnosis and management". J Am Acad Orthop Surg. 19 (6): 359–361. PMID 21628647.
- 1 2 3 4 Price, N (June 2008). "Prepatellar bursitis". Emergency Nurse. 16 (3): 20–24. doi:10.7748/en2008.06.16.3.20.c8183. PMID 18672851.
- ↑ Chatra, Priyank (January–March 2012). "Bursae around the knee joints". Ind J Radiol Imag. 22 (1): 27–30. doi:10.4103/0971-3026.95400. PMC 3354353. PMID 22623812.
- 1 2 Gonzales, R; Nadler, PL (2010). "Acute Knee Pain". In McPhee, SJ; Papadakis, MA. Current Medical Diagnosis & Treatment 2010. New York: McGraw-Hill Medical. p. 33. ISSN 0092-8682.
- ↑ Hellmann, DB; Imboden, JB (2010). "Bursitis". In McPhee, SJ; Papadakis, MA. Current Medical Diagnosis & Treatment 2010. New York: McGraw-Hill Medical. p. 743. ISSN 0092-8682.
- 1 2 Shiel, William C. "Bursitis of the Knee". MedicineNet. Retrieved 9 May 2012.
- 1 2 Schickendantz, MS; Watson, JT (September 1990). "Mycobacterial prepatellar bursitis". Clin Orthop Relat Res. 258 (258): 209–212. PMID 2203571.
- 1 2 "Prepatellar (Kneecap) Bursitis". American Academy of Orthopaedic Surgeons. July 2007. Retrieved 10 May 2012.
- ↑ Mysnyk, MC; et al. (January 1986). "Prepatellar bursitis in wrestlers". Am J Sports Med. 14 (1): 46–54. doi:10.1177/036354658601400109.
- ↑ Butcher JD, et al. (15 May 1996). "Lower extremity bursitis". Am Fam Physician. 53 (7): 2317–24. PMID 8638508.
- ↑ Hennrikus, WL; et al. (September 1989). "Treating septic prepatellar bursitis". West J Med. 151 (3): 331–332. PMC 1026890. PMID 2627225.
- ↑ Huang, Y; Yeh, W (March 2011). "Endoscopic treatment of prepatellar bursitis". Int Orthop. 35 (3): 355–358. doi:10.1007/s00264-010-1033-5.
- ↑ Allen, Kelly L (18 January 2012). "Prepatellar Bursitis". WebMD. Retrieved 21 May 2012.