Maternal physiological changes in pregnancy

Maternal physiological changes in pregnancy are the normal adaptations that a woman undergoes during pregnancy to better accommodate the embryo or fetus. They are physiological changes, that is, they are entirely normal, and include cardiovascular, hematologic, metabolic, renal and respiratory changes that become very important in the event of complications. The body must change its physiological and homeostatic mechanisms in pregnancy to ensure the fetus is provided for. Increases in blood sugar, breathing and cardiac output are all required. Levels of progesterone and estrogens rise continually throughout pregnancy, suppressing the hypothalamic axis and subsequently the menstrual cycle. The woman and the placenta also produce many hormones.
Hormonal
Pregnant women experience numerous adjustments in their endocrine system. Levels of progesterone and estrogens rise continually throughout pregnancy, suppressing the hypothalamic axis and subsequently the menstrual cycle. Estrogen is mainly produced by the placenta and is associated with fetal well–being. Women also experience increased human chorionic gonadotropin (β-hCG); which is produced by the placenta. This maintains progesterone production by the corpus luteum. The increased progesterone production, first by corpus luteum and later by the placenta, functions to relax bronchiolar smooth muscle. Elevated progesterone levels also contribute to an increase in minute ventilation to 50% greater than non-pregnant levels.
Prolactin levels increase due to maternal pituitary gland enlargement by 50%. This mediates a change in the structure of the mammary gland from ductal to lobular-alveolar. Parathyroid hormone is increased which leads to increases of calcium uptake in the gut and reabsorption by the kidney. Adrenal hormones such as cortisol and aldosterone also increase.
Human placental lactogen (hPL) is produced by the placenta and stimulates lipolysis and fatty acid metabolism by the woman, conserving blood glucose for use by the fetus. It can also decrease maternal tissue sensitivity to insulin, resulting in gestational diabetes.[1]
Body Weight

One of the most noticeable alterations in pregnancy is the gain in weight. The enlarging uterus, the growing fetus, the placenta and liquor amnii, the acquisition of fat and water retention, all contribute to this increase in weight. The weight gain varies from person to person and can be anywhere from 5 pounds (2.3 kg) to over 100 pounds (45 kg). In America, the doctor-recommended weight gain range is 25 pounds (11 kg) to 35 pounds (16 kg), less if the woman is overweight, more (up to 40 pounds (18 kg)) if the woman is underweight.
Breast size
A woman's breasts grow during pregnancy, usually 1 to 2 cup sizes and potentially several cup sizes. A woman who wore a C cup bra prior to her pregnancy may need to buy an F cup or larger bra while nursing.[2] A woman's torso also grows and her bra band size may increase one or two sizes.[3][4] An average of 80% of women wear the wrong bra size,[5] and mothers who are preparing to nurse can benefit from a professional bra fitting from a lactation consultant.[4] Once the baby is born and about 50 to 73 hours after birth, the mother will experience her breasts filling with milk (sometimes referred to as “milk coming in”) and at that point changes in the breast happen very quickly. Once lactation begins, the woman's breasts swell significantly and can feel achy, lumpy and heavy (which is referred to as engorgement). Her breasts may increase again in size, by another 1 or 2 cup sizes,[3][4] and individual breast size can vary daily or for longer periods depending on how much the infant nurses from each breast. A regular pattern of nursing is usually established after 8–12 weeks, and a woman's breasts will usually reduce in size, perhaps to about 1 cup size larger than prior to her pregnancy.[3] It has been shown, that changes in breast size during pregnancy could be associated with the sex of the infant. Mothers of female infants have greater changes in breast size than mothers of male infants.[6]
Many women and medical professionals[7][8] mistakenly think that breastfeeding causes their breasts to sag (medically referred to as ptosis),[9] and as a result some are reluctant to nurse their infants. In February 2009, Cheryl Cole told British Vogue that she hesitated to breastfeed because of the effect it might have on her breasts. "I want to breastfeed," she said, "but I’ve seen what it can do, so I may have to reconsider."[10] Research shows that breastfeeding is not the factor that many thought it was. The biggest factors affecting ptosis are cigarette smoking, a woman's body mass index (BMI), her number of pregnancies, her breast cup size before pregnancy, and age.[11][12]
Cardiovascular
During the course of pregnancy, blood volume slowly increases by 40–50%.[13] The increase is mainly due to an increase in plasma volume through increased aldosterone. It results in an increase in heart rate (15 beats/min more than usual), stroke volume, and cardiac output. Cardiac output increases by about 50%, mostly during the first trimester. The systemic vascular resistance also slightly decreases due to smooth muscle relaxation and overall vasodilation caused by elevated progesterone. Diastolic blood pressure consequently decreases between 12–26 weeks, and increases again to pre-pregnancy levels by 36 weeks. If the blood pressure becomes abnormally high, the woman should be investigated for pre-eclampsia and other causes of hypertension.
Cardiac function is also modified, with increased heart rate and increased stroke volume. A decrease in vagal tone and increase in sympathetic tone is the cause. Blood volume increases act to increase stroke volume of the heart via Starling's law. After pregnancy the change in stroke volume is not immediately reversed. Cardiac output rises from 4 to 7 liters in the 2nd trimester.
Haematology
During pregnancy the plasma volume increases by 50% and the red blood cell volume increases only by 20–30%.[13] Consequently, the hematocrit decreases on lab value; this is not a true decrease in hematocrit, however, but rather due to the dilution. The white blood cell count increases and may peak at over 20 mg/mL in stressful conditions. Conversely, there is a decrease in platelet concentration to a minimal normal values of 100-150 mil/mL.
A pregnant woman will also become hypercoagulable, leading to increased risk for developing blood clots and embolisms, due to increased liver production of coagulation factors, mainly fibrinogen and factor VIII (this hypercoagulable state along with the decreased ambulation (exercise involving legs) causes an increased risk of both DVT and PE). Women are at highest risk for developing clots, or thrombi, during the weeks following labor. Clots usually develop in the left leg or the left iliac venous system. The left side is most afflicted because the left iliac vein is crossed by the right iliac artery. The increased flow in the right iliac artery after birth compresses the left iliac vein leading to an increased risk for thrombosis (clotting) which is exacerbated by the aforementioned lack of ambulation following delivery. Both underlying thrombophilia and cesarean section can further increase these risks.
Edema, or swelling, of the feet is common during pregnancy, partly because the enlarging uterus compresses veins and lymphatic drainage from the legs.
Metabolic
During pregnancy, both protein metabolism and carbohydrate metabolism are affected. One kilogram of extra protein is deposited, with half going to the fetus and placenta, and another half going to uterine contractile proteins, breast glandular tissue, plasma protein, and haemoglobin.
An increased requirement for nutrients is given by fetal growth and fat deposition. Changes are caused by steroid hormones, lactogen, and cortisol.
Maternal insulin resistance can lead to gestational diabetes. Increased liver metabolism is also seen, with increased gluconeogenesis to increase maternal glucose levels.
Nutrition
Nutritionally, pregnant women require a caloric increase of 300 kcal/day and an increase in protein to 70 or 75 g/day. There is also an increased folate requirement from 0.4 to 0.8 mg/day (important in preventing neural tube defects). On average, a weight gain of 20 to 30 lb (9.1 to 13.6 kg) is experienced.
All patients are advised to take prenatal vitamins to compensate for the increased nutritional requirements. The use of Omega 3 fatty acids supports mental and visual development of infants.[14] Choline supplementation of research mammals supports mental development that lasts throughout life.[15]
Renal and lower reproductive tract
A pregnant woman may experience an increase in kidney and ureter size. The glomerular filtration rate (GFR) commonly increases by 50%, returning to normal around 20 weeks postpartum.[13] Plasma sodium does not change because this is offset by the increase in GFR. There is decreased blood urea nitrogen (BUN) and creatinine and glucosuria (due to saturated tubular reabsorption) may be seen. Persistent glucosuria may suggest gestational diabetes. The renin-angiotensin system is upregulated, causing increased aldosterone levels. Pregnancy alters the vaginal microbiota with a reduction in species/genus diversity.[16]
Gastrointestinal
During pregnancy, woman can experience nausea and vomiting (morning sickness); which may be due to elevated B-hCG and should resolve by 14 to 16 weeks. Additionally, there is prolonged gastric empty time, decreased gastroesophageal sphincter tone, which can lead to acid reflux, and decreased colonic motility, which leads to increased water absorption and constipation.
Immune tolerance
The fetus inside a pregnant woman may be viewed as an unusually successful allograft, since it genetically differs from the woman.[17] In the same way, many cases of spontaneous abortion may be described in the same way as maternal transplant rejection.[17]
Musculoskeletal
Neuromechanical adaptations to pregnancy refers to the change in gait, postural parameters, as well as sensory feedback, due to the numerous anatomical, physiological, and hormonal changes women experience during pregnancy. Such changes increase their risk for musculoskeletal disorders and fall injuries. Musculoskeletal disorders include lower-back pain, leg cramps, and hip pain. Pregnant women fall at a similar rate (27%) to women over age of 70 years (28%). Most of the falls (64%) occur during the second trimester. Additionally, two-thirds of falls are associated with walking on slippery floors, rushing, or carrying an object.[18] The root causes for these falls are not well known. However, some factors that may contribute to these injuries include deviations from normal posture, balance, and gait.
The body's posture changes as the pregnancy progresses. The pelvis tilts and the back arches to help keep balance. Poor posture occurs naturally from the stretching of the woman's abdominal muscles as the fetus grows. These muscles are less able to contract and keep the lower back in proper alignment. The pregnant woman has a different pattern of gait. The step lengthens as the pregnancy progresses, due to weight gain and changes in posture. On average, a woman's foot can grow by a half size or more during pregnancy. In addition, the increased body weight of pregnancy, fluid retention, and weight gain lowers the arches of the foot, further adding to the foot's length and width. The influences of increased hormones such as estrogen and relaxin initiate the remodeling of soft tissues, cartilage and ligaments. Certain skeletal joints such as the pubic symphysis and sacroiliac widen or have increased laxity.
The addition of mass, particularly around the torso, naturally changes a pregnant mother's center of mass (COM). The change in COM requires pregnant mothers to adjust their bodies to maintain balance.
Lumbar lordosis
To positionally compensate the additional load due to the pregnancy, pregnant mothers often extend their lower backs. As the fetal load increases, women tend to arch their lower backs, specifically in the lumbar region of their vertebral column to maintain postural stability and balance. The arching of the lumbar region is known as lumbar lordosis, which recovers the center of mass into a stable position by reducing hip torque. According to a study conducted by Whitcome, et al., lumbar lordosis can increase from an angle of 32 degrees at 0% fetal mass (i.e. non-pregnant women or very early in pregnancy) to 50 degrees at 100% fetal mass (very late in pregnancy). Postpartum, the angle of the lordosis declines and can reach the angle prior to pregnancy. Unfortunately, while lumbar lordosis reduces hip torque, it also exacerbates spinal shearing load,[19] which may be the cause for the common lower back pain experienced by pregnant women.[20]
Males vs. females
Given the demands of fetal loading during pregnancy and the importance of producing offspring to the fitness of human beings, one can imagine that natural selection has had a role in selecting a unique anatomy for the lumbar region in females. It turns out that there are sex differences in the lumbar vertebral column of human males and females, which ultimately helps mitigate some of the discomfort due to the fetal load in females. There are 5 vertebrae in the lumbar region for both males and females. However, the 3 lower vertebrae of a female's lumbar region are dorsally wedged while for males, only the lower 2 of the lumbar region are dorsally wedged. When a female arches her lower back, such as during fetal loading, having an extra dorsally wedged vertebra lessens the shearing force. This lumbar sexual dimorphism in humans suggests high natural selection pressures have been acting to improve maternal performance in posture and locomotion during pregnancy.[19]
Evolutionary implication
If natural selection has acted on the lumbar region of Homo Sapiens to create this sexual dimorphism, then this sort of trait should also be apparent in the genus Australopithecus, hominins that have been known to be habitually bipedal for at least 2 million years after the earliest bipedal hominins. Currently there are 2 nearly complete australopith lumbar segments; one has three dorsally wedged vertebrae in the lumbar region while the other has two. An explanation for these findings is that the first one is a female, while the latter is a male. This sort of evidence supports the notion that natural selection has played a dimorphic role in designing the anatomy of the vertebral lumbar region.[19]
Postural stability
The weight added during the progression of pregnancy also affects the ability to maintain balance. In biomechanics, balance refers to one’s ability to maintain the center of gravity within the base of support with minimal postural sway. In other words, the moment (or torque) generated by gravity must be balanced by the ankle moment in order to maintain postural stability. Although quiet standing appears to be static, it is actually a process of rocking from the ankle in the sagittal plane.[21]
Maintenance
Currently, there are 3 main hypotheses suggesting how humans maintain postural stability while standing.
- Stiffness of ankle joint: The stiffness model was first introduced by Winter et al., in 1998,[22] and states that simple stiffness of ankle muscles account for the control of balance during quiet standing. The stiffness of the ankle muscle was determined experimentally by summing up the moments (or torque) left and right about the ankle and dividing it by the sway angle (angle at which the center of mass is displaced from the center of pressure). It was found in both analytical and experimental data (using human subjects) that there was a linear relationship between moments about the ankle muscle and sway angle. Additionally, the stiffness (i.e. total moment divided by sway angle) was found to be very close to 1, indicating a resemblance between the ankle joint and a perfect spring.
- Moment arm of ankle muscles: The moment arm of ankle muscle hypothesis for postural stability was first developed in 1993 by Young et al.[23] and has been primarily seen in cats, though it is speculated that such mechanisms may also exist in humans. Results obtained from Young et al. showed that in the cat ankle joint, many of its muscles have predominant moment arms about the adduction/abduction axis. Smaller moment arms are found in inversion/eversion and about the principal axis of motion, dorsiflexion/extension. Additionally, Young et al. showed that the magnitudes of the moment arms in abduction/adduction and inversion/eversion strongly depended on joint angle. As the joint angle moved increasingly away from the neutral axis, the magnitude of the moment arms also increased. Such a finding suggests that, at least in cats, the coactivation of these agonist-antagonistmuscles is used for immediate stabilization in posture.
- Proprioception: Proprioception means "sense of self". In limbs, proprioceptors are sensors that provide information about joint angle, muscle length, and tension, which is integrated to give information about the position of the limb in space. For postural stability, it has been suggested that stretch receptors may contribute to immediate stabilization in posture. However, researchers have found a weak correlation between muscle length and ankle joint angle, indicating that the stretch reflex is probably not the main contributor to postural stability. Additionally, there is approximately a 30 ms time delay between any stretch receptor response to a change in muscle length, which further supports the idea that stretch receptors may not have a big contribution to postural stability. However, this should not rule out the role of all proprioceptors in maintaining postural stability in humans.[24][25]
While these are the three leading hypotheses, of course there is always a possibility that there is a combination of all mechanisms that ultimately allows humans to maintain postural stability during quiet standing. Additionally, it is important to keep in mind that there are also many physiological factors such as weight, internal noise to muscles, etc. that may come into play when trying to understand the factors that contribute to postural stability.
Perception
Pregnant women have a decreased perception of balance during quiet standing, which is confirmed by an increase in anterior-posterior sway.[26] This relationship heightens as pregnancy progresses and significantly decreases post-partum. To compensate for the decrease in balance stability (both actual and perceived), stance width increases to maintain postural stability.
Response to perturbations
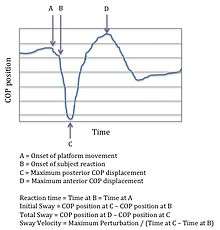
Under dynamic postural stability, which can be defined as the response to anterior (front) and posterior (back) translation perturbations, the effects of pregnancy are different. Initial sway, total sway, and sway velocity (see figure for description of variables) are significantly less during the third trimester than during the second trimester and when compared to non-pregnant women. These biomechanical characteristics are possible reasons why falls are more prevalent during the second trimester during pregnancy.
Additionally, the time it takes for pregnant women (any stage of pregnancy) to react to a translational disturbance is not significantly different than that of non-pregnant women.[27] This alludes to some sort of stability mechanism that allow pregnant women to compensate for the changes they experience during pregnancy.
Gait
Gait in pregnant women often appear as a “waddle” – a forward gait that includes a lateral component. However, research has shown that the forward gait alone remains unchanged during pregnancy. It has been found that gait parameters such as gait kinematics, (velocity, stride length, and cadence) remain unchanged during the third trimester of pregnancy and 1 year after delivery. These parameters suggest that there is no change in forward movement. There is, though, a significant increases in kinetic gait parameters, which may be used to explain how gait motion remains relatively unchanged despite increase in body mass, width and changes in mass distribution about the waist during pregnancy. These kinetic gait parameters suggest an increased use of hip abductor, hip extensor, and ankle plantar flexor muscle groups. To compensate for these gait deviations, pregnant women often make adaptations that can result in musculoskeletal injuries. While the idea of "waddling" cannot be dispensed, these results suggest that exercise and conditioning may help relieve these injuries.[28]
Respiratory
Progesterone has noticeable effects on respiratory physiology, increasing minute ventilation by 40% in the first trimester.[29]
See also
References
- ↑ "Gestational Diabetes in Primary Care: Diabetes in Pregnancy, Medscape". Retrieved 2011-06-22.
- ↑ "Nursing bras". Consumer Reports. Retrieved 16 November 2011.
- 1 2 3 "Frequently Asked Questions". BravadoDesigns.com. Retrieved 24 November 2011.
- 1 2 3 "Nursing bras". Consumer Reports. Retrieved 16 November 2011.
- ↑ Wood K, Cameron M, Fitzgerald K (2008). "Breast Size, Bra Fit and Thoracic Pain in Young Women: A Correlational Study". Chiropractic & Osteopathy. 16: 1. doi:10.1186/1746-1340-16-1. PMC 2275741
 . PMID 18339205.
. PMID 18339205. - ↑ Galbarczyk A (2011). "Unexpected changes in maternal breast size during pregnancy in relation to infant sex: an evolutionary interpretation.". American Journal of Human Biology. 23: 560–2. doi:10.1002/ajhb.21177. PMID 21544894.
- ↑ Lauersen, Niels H.; Stukane, Eileen (1998). The Complete Book of Breast Care (1st Trade Paperback ed.). New York: Fawcett Columbine/Ballantine. ISBN 978-0-449-91241-6.
- ↑ "Breast Sagging". Retrieved 2 February 2012.
- ↑ "Sagging Breasts". Channel 4. 2009. Retrieved 3 February 2012.
- ↑ Jay, Elizabeth (February 13, 2009). "Will breastfeeding leave you with a little less lift?". Retrieved 2 February 2012.
- ↑ Thompson, Andrea (November 2, 2007). "Breastfeeding Does Not Make Breasts Sag, Study Suggests". LiveScience.com. Retrieved 2 February 2012.
- ↑ Campolongo, Marianne (December 5, 2007). "What Causes Sagging Breasts?". Retrieved 26 January 2012.
- 1 2 3 Guyton and hall (2005). Textbook of Medical Physiology (11 ed.). Philadelphia: Saunders. pp. 103g. ISBN 81-8147-920-3.
- ↑ "Omega-3 least known of pregnancy "Big 3"". Retrieved 2008-01-01.
- ↑ Tees RC, Mohammadi E (1999). "The effects of neonatal choline dietary supplementation on adult spatial and configural learning and memory in rats". Dev Psychobiol. 35 (3): 226–40. doi:10.1002/(SICI)1098-2302(199911)35:3<226::AID-DEV7>3.0.CO;2-H. PMID 10531535.
- ↑ Clark, Natalie; Tal, Reshef; Sharma, Harsha; Segars, James (2014). "Microbiota and Pelvic Inflammatory Disease". Seminars in Reproductive Medicine. 32 (01): 043–049. doi:10.1055/s-0033-1361822. ISSN 1526-8004. PMC 4148456. PMID 24390920.
- 1 2 Clark DA, Chaput A, Tutton D (March 1986). "Active suppression of host-vs-graft reaction in pregnant mice. VII. Spontaneous abortion of allogeneic CBA/J x DBA/2 fetuses in the uterus of CBA/J mice correlates with deficient non-T suppressor cell activity". J. Immunol. 136 (5): 1668–75. PMID 2936806.
- ↑ Dunning, K., Lemasters, G., Levin, L., Battacharya, A., Alterman, T., Lord, K., 2003. Falls in workers during pregnancy: risk factors, job hazards, and high risk occupations. Am. J. Ind. Med. 44, 664-672.
- 1 2 3 Whitcome K.K.; Shapiro L.J.; Lieberman D.E. (2007). "Fetal load and the evolution of lumbar lordosis in bipedal hominins". Nature. 450: 1075–1078. doi:10.1038/nature06342. PMID 18075592.
- ↑ Ostgaard HC, Andersson GB, Karlsson K (1991). "Prevalence of back pain in pregnancy". Spine. 16 (5): 549–52. doi:10.1097/00007632-199105000-00011. PMID 1828912.
- ↑ Masani, K., Popovic, M.R., Nakazaqa, K., Kouzaki, M., Nozaki, D. 2033. Importance of body sway velocity information in controlling ankle extensor activities during quiet stance. Journal of Neurophysiology. 90, 3774-3782.
- ↑ Winter D.A.; Patla A.E.; Rietdyk S.; Ishac M.G. (2001). "Ankle Muscle Stiffness in the Control of Balance During Quiet Standing". Journal of Neurophysiology. 85: 2630–2633.
- ↑ Young, R.P., G.E. Loeb. "The distal hindlimb musculature of the cat: multiaxis moment arms at the ankle joint". Exp Brain Res (1993) 96:141-151.
- ↑ Bloem B.R.; Allum J.H.J.; Carpenter M.G. (2000). "Is lower leg proprioception essential for triggering human automatic postural responses?". Exp Brain Res. 130: 375–391. doi:10.1007/s002219900259.
- ↑ Bloem B.R.; Allum J.H.J.; Carpenter M.G.; Verschuuren J.J.G.M.; Honegger F. (2002). "Triggering of balance corrections and compensatory strategies in a patient with total leg proprioceptive loss". Exp Brain Res. 142: 91–107. doi:10.1007/s00221-001-0926-3.
- ↑ Jang, J., Hsiao, K.T., Hsiao-Wecksler, E., 2008. Balance (perceived and actual) and preferred stance width during pregnancy. Clinical Biomechanics. 23, 468-476.
- ↑ J.L. McCrory, Chambers, A.J., Daftary, A., Redfern, M.S., 2010. Dynamic postural stability during advancing pregnancy. Journal of Biomechanics. 43, 2434-2439.
- ↑ Foti, T., Davids, J.R., Bagley, A., 2000. A biomechanical analysis of gait during pregnancy. The Journal of Bone and Joint Surgery. 82-A, 625-632.
- ↑ Campbell, LA; Klocke, RA (April 2001). "Implications for the pregnant patient.". American Journal of Respiratory and Critical Care Medicine. 163 (5): 1051–54. doi:10.1164/ajrccm.163.5.16353. PMID 11316633.