Poland syndrome
| Poland syndrome | |
|---|---|
| Synonyms | Poland's syndrome, Poland's syndactyly, Poland sequence,[1] Poland's anomaly |
 | |
| Digital mammogram (Mediolateral view) showing absence of the pectoralis major muscle and architectural distortion on the left side and normal right breast | |
| Classification and external resources | |
| Specialty | medical genetics |
| ICD-10 | Q79.8 |
| ICD-9-CM | 756.89 |
| OMIM | 173800 |
| DiseasesDB | 31679 |
| eMedicine | plastic/132 |
| MeSH | D011045 |
Poland syndrome is a rare birth defect characterized by underdevelopment or absence of the chest muscle (pectoralis) on one side of the body, and usually also webbing of the fingers (cutaneous syndactyly) of the hand on the same side (the ipsilateral hand).[2] In most affected individuals, the missing part is the large section of the muscle that normally attaches to the upper arm on one side and the breastbone (sternum) on the other. Other abnormalities may occur on the affected side of the torso. In some cases, additional muscles in the chest wall, side, and shoulder are missing or underdeveloped.
There may also be rib cage abnormalities, such as shortened ribs, and the ribs may be noticeable due to less fat under the skin (subcutaneous fat). Breast and nipple abnormalities may also occur, and underarm (axillary) hair is sometimes sparse or abnormally placed. In most cases, the abnormalities in the chest area do not cause health problems or affect movement.[3] Poland syndrome most often affects the right side of the body, and occurs more often in males than in females.
It is usually considered a unilateral condition. Some have claimed that the term can be applied in bilateral presentation,[4] but others recommend using alternate terminology in those cases.[5]
Signs and symptoms
Very frequent signs
- Abnormal gastrointestinal tract
- Absent pectoral muscles
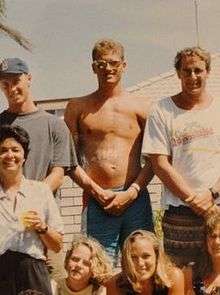 Male showing left pectoral absent
Male showing left pectoral absent - Brachydactyly (Short fingers)
- Dextrocardia
- Diaphragmatic hernia/defect
- Humerus absent/abnormal
- Liver/biliary tract anomalies
- Maternal diabetes
- Oligodactyly/missing fingers
- Radius absent/abnormal
- Rhizomelic micromelia (relatively shorter proximal segment of the limbs compared to the middle and the distal segments)
- Sparcity or abnormality of axillary hair on affected side
- Syndactyly of fingers (webbing)
- Ulna absent/abnormal
- Upper limb asymmetry
- Abnormal rib
- Simian crease on affected side
Frequent signs
- Hypoplastic/absent nipples
- Scapula anomaly
Occasional signs
- Agenesis/hypoplasia of kidneys
- Encephalocele/exencephaly
- Abnormal morphology of hypothalamic-hypophyseal axis
- Abnormal function of hypothalamic-hypophyseal axis
- Microcephaly
- Preaxial polydactyly
- Ureteric anomalies (reflux/duplex system)
- Vertebral segmentation anomaly
Causes
The cause of Poland syndrome is unknown. However, an interruption of the embryonic blood supply to the arteries that lie under the collarbone (subclavian arteries) at about the 46th day of embryonic development is the prevailing theory.[6]
The subclavian arteries normally supply blood to embryonic tissues that give rise to the chest wall and hand. Variations in the site and extent of the disruption may explain the range of signs and symptoms that occur in Poland syndrome. Abnormality of an embryonic structure called the apical ectodermal ridge, which helps direct early limb development, may also be involved in this disorder. Rare cases of Poland syndrome are thought to be caused by a genetic change that can be passed down in families, but no related genes have been identified.[7]
Treatment


Technique
The complete or partial absence of the pectoralis muscle, is the malformation that defines Poland Syndrome. It can be treated by the insertion of a custom implant designed by CAD (computer aided design).[8] A 3D reconstruction of the patient's chest is performed from a medical scanner, to design a virtual implant perfectly adapted to the anatomy of each one.[9] The implant is made of medical silicone unbreakable rubber.
The Poland syndrome malformations being morphological, correction by custom implant is a first-line treatment.[10] This technique allows a wide variety of patients to be treated with good outcomes. Poland Syndrome can be associated with bones, subcutaneous and mammary atrophy: if the first, as for pectus excavatum, is successfully corrected by a custom implant, the others can require surgical intervention such as lipofilling or silicone breast implant, in a second operation.

Surgery
The surgery takes place under general anaesthesia and lasts less than 1 hour. The surgeon prepares the locus to the size of the implant after performing a 8-cm axillary incision and inserts the implant beneath the skin. The closure is made in 2 planes.
The implant will replace the pectoralis major muscle, thus enabling the thorax to be symmetrical and, in women, the breast as well. If necessary, especially in the case of women, a second operation will complement the result by the implantation of a breast implant and / or lipofilling .
Surgical outcomes
Good surgical outcomes are easily achievable; the pain is treated with simple analgesics.
Minimal post-operative care: the stitches are resorbable, no drain is required, only a dressing for 8 days and a compression bra to wear from discharge for 15 days. Follow‑up consultation has to be done after 8 days. Sick leave is recommended for 15 days and playing sport can be resumed after 3 months.
Epidemiology
According to the National Human Genome Research Institute, Poland syndrome affects males three times as often as females and affects the right side of the body twice as often as the left.[11] The incidence is estimated to range from one in 7,000 to one in 100,000 live births.[12]
History

It was first named in 1962 by Patrick Clarkson, a New Zealand-born British plastic surgeon working at Guy's Hospital and Queen Mary's Hospital, London. He noticed that three of his patients had both a hand deformity and an underdeveloped breast on the same side. He discussed this with his colleague at Guy's Hospital, Dr Philip Evans, who agreed that the syndrome was "not widely appreciated". Clarkson found a reference to a similar deformity published by Alfred Poland, over a hundred years earlier in Guy's Hospital reports, in 1841.[13] Clarkson was able to find the hand specimen dissected by Poland, which was still held in the hospital pathology museum.
Poland had dissected a convict known as George Elt, who was said to be unable to draw his hand across his chest. Poland noted the chest wall deformity, and this was illustrated in his article; the hand was also dissected and preserved for posterity in Guy's Hospital museum where it remains today. It cannot be truly said that Poland described this syndrome because he only described one isolated case. Clarkson published his series of three cases and named the syndrome after Poland in his article.[14]
Notable cases
British TV presenter Jeremy Beadle (1948–2008) was known for having this condition. His Poland Syndrome manifested itself in the form of his disproportionately small right hand.[15]
Olympic boxer Jérôme Thomas is also affected by Poland syndrome as his left arm and hand are significantly shorter and smaller than his right. Thomas also lacks a left pectoral muscle.
PGA Tour golfer Bryce Molder has Poland syndrome with an absent left pectoral muscle and a small left hand. Several surgeries in his childhood repaired syndactly on the left hand.[16]
Actor Ted Danson, famous for starring in the TV show Cheers, admitted he had the condition in 2000 to Orange Coast magazine, and said that he was bullied as a child because of it.[17]
Formula One World Champion Fernando Alonso is affected by Poland syndrome - he is missing the right pectoral muscle.[18]
English cricketer Lewis Hatchett was born with Poland syndrome.[19]
Researchers from the Department of Rehabilitation Medicine at the Yonsei University College of Medicine in Seoul, Korea reported a case of congenital absence of pectoralis major in 1990. According to Kakulas and Adams, pectoralis major is the most frequently congenitally absent muscle. The case involved a 22-year-old marine who had asymmetrical configuration of chest wall who had never experienced difficulties performing daily activities, but who experienced difficulties in the military camp. He had difficulty in some training activities especially those such as throwing a grenade or rope climbing.
References
- ↑ Martínez-Frías ML, Czeizel AE, Rodríguez-Pinilla E, Bermejo E (January 1999). "Smoking during pregnancy and Poland sequence: results of a population-based registry and a case-control registry". Teratology. 59 (1): 35–8. doi:10.1002/(SICI)1096-9926(199901)59:1<35::AID-TERA8>3.0.CO;2-E. PMID 9988881.
- ↑ "Poland Syndrome". NORD (National Organization for Rare Disorders). Retrieved 2016-02-29.
- ↑ "Poland Syndrome". Genetics Home Reference. Retrieved 12 December 2014.
- ↑ Karnak I, Tanyel FC, Tunçbilek E, Unsal M, Büyükpamukçu N (February 1998). "Bilateral Poland anomaly". Am. J. Med. Genet. 75 (5): 505–7. doi:10.1002/(SICI)1096-8628(19980217)75:5<505::AID-AJMG9>3.0.CO;2-L. PMID 9489794.
- ↑ Maroteaux P, Le Merrer M (December 1998). "Bilateral Poland anomaly versus thoracic dysplasia". Am. J. Med. Genet. 80 (5): 538–9. doi:10.1002/(SICI)1096-8628(19981228)80:5<538::AID-AJMG23>3.0.CO;2-S. PMID 9880227.
- ↑ Poullin P, Toussirot E, Schiano A, Serratrice G (1992). "[Complete and dissociated forms of Poland's syndrome (5 cases)]". Rev Rhum Mal Osteoartic. 59 (2): 114–20. PMID 1604222.
- ↑ "Poland Syndrome". Genetics Home Reference. Retrieved 12 December 2014.
- ↑ J-P. Chavoin; A.André; E.Bozonnet; A.Teisseyre; J. Arrue; B. Moreno; D. Glangloff; J-L. Grolleau; I.Garrido (2010). "Mammary implant selection or chest implants fabrication with computer help". Annales de chirurgie plastique esthétique. 55: 471–480.
- ↑ "anatomikmodeling.com".
- ↑ Chichery A.; Jalbert F.; Foucras L.; Grolleau J.-L.; Chavoin J.-P. (2006). "Syndrome de Poland". EMC - Techniques chirurgicales - Chirurgie plastique reconstructrice et esthétique. 1 (3): 1. doi:10.1016/S1286-9325(06)44494-0.
- ↑ "Learning about Poland Anomaly". Retrieved 2007-02-09.
- ↑ Fokin A, Robicsek F (2002). "Poland's syndrome revisited". Ann Thorac Surg. 74 (6): 2218–25. doi:10.1016/S0003-4975(02)04161-9. PMID 12643435.
- ↑ Poland A (1841). "Deficiency of the pectoral muscles". Guy's Hospital Reports. VI: 191–193.
- ↑ Clarkson P (1962). "Poland's syndactyly". Guys Hosp Rep. 111: 335–46. PMID 14021589.
- ↑ Burt, Jennifer (1997-10-20). "Jeremy is a role model for children". Leicester (UK) Mercury.
- ↑ "Bryce Molder". PGA Tour. Archived from the original on January 6, 2011. Retrieved 6 Jan 2011.
- ↑ https://books.google.co.uk/books?id=yAQEAAAAMBAJ&pg=PA36&lpg=PA36#v=onepage&q&f=false
- ↑ "Poland Syndrome". Dovemed. Retrieved 31 Mar 2016.
- ↑ "Hatchett retires after defying the odds". ESPN Cricinfo. Retrieved 24 September 2016.
External links
- Poland Syndrome Charity - exists to support those who need information and help dealing with Poland Syndrome