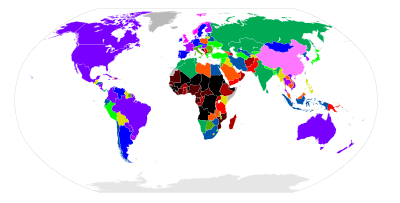
Prevalence of birth control
|
6%
12%
18%
24%
30%
36%
|
42%
48%
54%
60%
66%
72%
|
78%
84%
86%
No data
|
Globally approximately 45% of those who are married and able to have children use contraception.[1] As of 2007, IUDs were used by about 17% of women of child bearing age in developing countries and 9% in developed countries or more than 180 million women worldwide.[2] Avoiding sex when fertile is used by about 3.6% of women of childbearing age, with usage as high as 20% in areas of South America.[3] As of 2005, 12% of couples are using a male form of contraception (either condoms or a vasectomy) with rates of up to 30% in the developed world.[4]
As of 2012, 57% of women of child bearing age wanted to avoid pregnancy (867 of 1520 million).[5] About 222 million women however were not able to access birth control, 53 million of whom were in sub-Saharan Africa and 97 million of whom were in Asia.[5] Many countries limit access to birth control due to the religious and political reasons.[6]
Africa
Contraceptive use among women in Sub-Saharan Africa has risen from about 5% in 1991 to about 30% in 2006.[7] However, due to extreme poverty, lack of access to birth control, and restrictive abortion laws, many women still resort to clandestine abortion providers for unintended pregnancy, resulting in about 3% obtaining unsafe abortions each year.[8][9] South Africa, Botswana, and Zimbabwe have successful family planning programs, but other central and southern African countries continue to encounter extreme difficulties in achieving higher contraceptive prevalence and lower fertility for a wide variety of compounding reasons.[10]
China
The one-child policy of the People's Republic of China requires couples to have no more than one child. Beginning in 1979, the policy was implemented to control rapid population growth.[11] Chinese women receive free contraception and family planning services.[12] Greater than 70% of those of childbearing age use contraception.[1] Since the policy was put into place in 1979, over 400 million births have been prevented.[12] Because of various exemptions, fertility rate is about 1.7 children per woman, down from 5.9 in the 1960s. A strong preference for boys and free access to fetus sex determination and abortion has resulted in an artificially high proportion of males in both rural and urban areas.[12]
India
Awareness of contraception is near-universal among married women in India.[13] However, the vast majority of married Indians (76% in a 2009 study) reported significant problems in accessing a choice of contraceptive methods.[14] In 2009, 48.3% of married women were estimated to use a contraceptive method, i.e. more than half of all married women did not.[14] About three-fourths of these were using female sterilization, which is by far the most prevalent birth-control method in India.[14] Condoms, at a mere 3%, were the next most prevalent method.[14] Meghalaya, Bihar and Uttar Pradesh had the lowest usage of contraception among all Indian states with rates below 30%.[14]
Pakistan
In 2011 just one in five Pakistani women aged 15 to 49 used modern birth control.[15] In 1994, Pakistan pledged that by 2010 it would provide universal access to family planning.[16] but contraception is shunned under traditional social norms.[15] Most women who say they do not want any more children or would like to wait a period of time before their next pregnancy do not have the contraceptive resources available to them in order to do so.[16] In the 1990s, women increasingly reported wanting fewer children, and 24 percent of recent births were reported to be unwanted or mistimed.[16] The rate of unwanted pregnancies is higher for women living in poor or rural environments; with two-thirds of women live in rural areas.[16] While 96 percent of married women were reported to know about at least one method of contraception, only half of them had ever used it.[16] The most commonly reported reasons for married women electing not to use family planning methods include the belief that fertility should be determined by God (28%); opposition to use by the woman, her husband, others or a perceived religious prohibition (23%); infertility (15%); and concerns about health, side effects or the cost of family planning (12%).[16]
United Kingdom
Contraception has been available for free under the National Health Service since 1974, and 74% of reproductive age women use some form of contraception.[17] The levonorgestrel intrauterine system has been massively popular.[17] Sterilization is popular in older age groups, among those 45-49, 29% of men and 21% of women have been sterilized.[17] Female sterilization has been declining since 1996, when the intrauterine system was introduced.[17] Emergency contraception has been available since the 1970s, a product was specifically licensed for emergency contraception in 1984, and emergency contraceptives became available over the counter in 2001.[17] Since becoming available over the counter it has not reduced the use of other forms of contraception, as some moralists feared it might.[17] In any year only 5% of women of childbearing age use emergency hormonal contraception.[17] Despite widespread availability of contraceptives, almost half of pregnancies were unintended circa 2005.[17] Abortion was legalized in 1967.[17]
United States
In the United States 98% of women have used birth control at some point in time and 62% of those of reproductive age are currently using birth control.[6] The two most common methods are the pill (11 million) and sterilization (10 million).[6] Despite the availability of highly effective contraceptives, about half of US pregnancies are unintended.[18] In the United States, contraceptive use saves about $19 billion in direct medical costs each year.[18] Usage of the IUD has more than tripled between 2002 and 2011 in the United States. In 2011, IUDs made up 10% of all birth control methods, with women increasingly viewing the IUD as the most convenient, safe, and effective yet reversible form of contraception.[19]
References
- 1 2 Darney, Leon Speroff, Philip D. (2010). A clinical guide for contraception (5th ed.). Philadelphia, Pa.: Lippincott Williams & Wilkins. p. 10. ISBN 1-60831-610-6.
- ↑ Darney, Leon Speroff, Philip D. (2010). A clinical guide for contraception (5th ed.). Philadelphia, Pa.: Lippincott Williams & Wilkins. pp. 242–243. ISBN 9781608316106.
- ↑ Darney, Leon Speroff, Philip D. (2010). A clinical guide for contraception (5th ed.). Philadelphia, Pa.: Lippincott Williams & Wilkins. p. 315. ISBN 1-60831-610-6.
- ↑ Naz, RK; Rowan, S (June 2009). "Update on male contraception.". Current opinion in obstetrics & gynecology. 21 (3): 265–9. doi:10.1097/gco.0b013e328329247d. PMID 19469045.
- 1 2 Darroch, JE; Singh, S (May 18, 2013). "Trends in contraceptive need and use in developing countries in 2003, 2008, and 2012: an analysis of national surveys.". Lancet. 381 (9879): 1756–1762. doi:10.1016/S0140-6736(13)60597-8. PMID 23683642.
- 1 2 3 Hurt, K. Joseph; et al., eds. (2012-03-28). The Johns Hopkins manual of gynecology and obstetrics (4th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. p. 232. ISBN 978-1-60547-433-5.
- ↑ Cleland, JG; Ndugwa, RP; Zulu, EM (Feb 1, 2011). "Family planning in sub-Saharan Africa: progress or stagnation?". Bulletin of the World Health Organization. 89 (2): 137–43. doi:10.2471/BLT.10.077925. PMC 3040375
 . PMID 21346925.
. PMID 21346925. - ↑ Rasch, V (July 2011). "Unsafe abortion and postabortion care - an overview.". Acta Obstetricia et Gynecologica Scandinavica. 90 (7): 692–700. doi:10.1111/j.1600-0412.2011.01165.x. PMID 21542813.
- ↑ Huezo, CM (August 1998). "Current reversible contraceptive methods: a global perspective.". International journal of gynaecology and obstetrics: the official organ of the International Federation of Gynaecology and Obstetrics. 62 Suppl 1: S3–15. doi:10.1016/s0020-7292(98)00084-8. PMID 9806233.
- ↑ Lucas, D (May–Jun 1992). "Fertility and family planning in southern and central Africa.". Studies in family planning. 23 (3): 145–58. doi:10.2307/1966724. PMID 1523695.
- ↑ Kane, P.; Choi, C. Y. (Oct 9, 1999). "China's one child family policy". BMJ (Clinical research ed.). 319 (7215): 992–4. doi:10.1136/bmj.319.7215.992. PMC 1116810. PMID 10514169.
- 1 2 3 Hesketh, T.; Lu, L.; Xing, Z. W. (Sep 15, 2005). "The effect of China's one-child family policy after 25 years". The New England Journal of Medicine. 353 (11): 1171–6. doi:10.1056/NEJMhpr051833. PMID 16162890.
- ↑ B.M. Ramesh; S.C. Gulati; R.D. Retherford. "Contraceptive use in India, 1992–93" (PDF). National Family Health Survey Subject Reports, Number 2, October 1996. International Institute for Population Sciences. Retrieved 2009-11-25
- 1 2 3 4 5 "India and Family Planning: An Overview" (PDF). Department of Family and Community Health, World Health Organization. Retrieved 2009-11-25
- 1 2 Brulliard, Karin (15 December 2011). "As Pakistan's population soars, contraceptives remain a hard sell". The Washington Post. Retrieved 19 April 2012.
- 1 2 3 4 5 6 Hardee, Karen and Leahy, Elizabeth. "Population, Fertility and Family Planning in Pakistan: A Program in Stagnation." Population Action International. Volume 4, Number 1, 1-12. 2007.
- 1 2 3 4 5 6 7 8 9 Rowlands S (October 2007). "Contraception and abortion". J R Soc Med. 100 (10): 465–8. doi:10.1258/jrsm.100.10.465. PMC 1997258. PMID 17911129.
- 1 2 James Trussell, Anjana Lalla, Quan Doan, Eileen Reyes, Lionel Pinto, Joseph Gricar (2009). "Cost effectiveness of contraceptives in the United States". Contraception. 79 (1): 5–14. doi:10.1016/j.contraception.2008.08.003. PMC 3638200. PMID 19041435.
- ↑ "Jane Brody on IUDs - NYTimes.com". Retrieved 2012-02-28.