Seborrhoeic dermatitis
| Seborrheic dermatitis | |
|---|---|
| Synonyms | seborrhea, sebopsoriasis, seborrheic eczema, pityriasis capitis[1] |
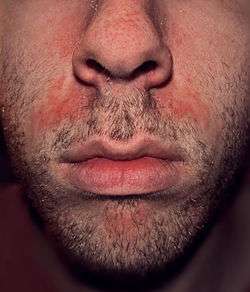 | |
| An example of seborrhoeic dermatitis between the nose and mouth | |
| Classification and external resources | |
| Specialty | Dermatology |
| ICD-10 | L21 |
| ICD-9-CM | 690.1 |
| DiseasesDB | 11911 |
| MedlinePlus | 000963 |
| eMedicine | derm/396 |
| MeSH | D012628 |
Seborrheic dermatitis, also known as seborrheic eczema or simply as seborrhea, is a chronic, relapsing and usually mild dermatitis. In infants seborrheic dermatitis is called cradle cap. Dandruff is a type of seborrhoeic dermatitis where inflammation is not present.[2] Seborrheic dermatitis is a skin disorder affecting the scalp, face, and torso. Typically, seborrheic dermatitis presents with scaly, flaky, itchy, and red skin. It particularly affects the sebaceous-gland-rich areas of skin. In adolescents and adults, seborrhoeic dermatitis usually presents as scalp scaling or as redness of the nasolabial fold.
The topical antifungal medications ketoconazole and ciclopirox are both effective for the condition.[3] It is unclear if other antifungals are equally effective as this has not been studied.[3]
Signs and symptoms


Seborrhoeic dermatitis' symptoms appear gradually and usually the first signs are flaky skin and scalp.[4] Symptoms occur most commonly anywhere on the skin of the face, behind the ears and in areas where the skin folds. Flakes may be yellow, white or grayish.[5] Redness and flaking may also occur on the skin near the eyelashes, on the forehead, around the sides of the nose, and the chest and upper back.
In more severe cases, yellowish to reddish scaly pimples appear along the hairline, behind the ears, in the ear canal, on the eyebrows, on the bridge of the nose, around the nose, on the chest, and on the upper back.[6]
Commonly, patients experience mild redness, scaly skin lesions and in some cases hair loss.[7] Other symptoms include patchy scaling or thick crusts on the scalp, red, greasy skin covered with flaky white or yellow scales, itching, soreness and yellow or white scales that may attach to the hair shaft.[8]
Seborrheic dermatitis can occur in infants younger than three months and it causes a thick, oily, yellowish crust around the hairline and on the scalp. Itching is not common among infants. Frequently, a stubborn diaper rash accompanies the scalp rash.[6] Usually, when it occurs in infants the condition resolves itself within days and with no treatment.
In adults, symptoms of seborrheic dermatitis may last from a few weeks, to years. Many patients experience alternating periods of inflammation. The condition is referred to a specialist when self-care has proven unsuccessful.
Causes
The specific causes are not known.[9] Current theories for the cause of the disease include a weakened immune system, the lack of specific nutrients (for example zinc), or issues with the nervous system.[10]
Fungal
Seborrhoeic dermatitis may involve an inflammatory reaction to a proliferation of a form of the yeast Malassezia,[11][12] though this has not been proven.[13]
The main species found on the scalp is Malassezia globosa, others being Malassezia furfur (formerly known as Pityrosporum ovale) and Malassezia restricta. The yeast produces toxic substances that irritate and inflame the skin. Patients with seborrhoeic dermatitis appear to have a reduced resistance to the yeast. However, the colonization rate of affected skin may be lower than that of unaffected skin.[14]
Only saturated fatty acids (FAs) have been shown to support Malassezia growth. It has also been shown that while number density of M. globosa and M. restricta do not directly correlate to dandruff presence or severity, removal correlates directly with amelioration of flaking. Furthermore, in dandruff-susceptible individuals pure oleic acid, an unsaturated FA and Malassezia metabolite, induces flaking in the absence of Malassezia by direct effects on the host skin barrier. These findings support the following hypothesis:
Malassezia hydrolyze human sebum, releasing a mixture of saturated and unsaturated fatty acids. They take up the required saturated FAs, leaving behind unsaturated FAs. The unsaturated FAs penetrate the stratum corneum. Because of their non-uniform structure, they breach the skin's barrier function. This barrier breach induces an irritation response, leading to dandruff and seborrheic dermatitis.[15]
Other
Genetic, environmental, hormonal, and immune-system factors have been shown to be involved in the manifestation of seborrhoeic dermatitis.[16][17]
Seborrhoeic dermatitis may be aggravated by illness, psychological stress, fatigue, sleep deprivation, change of season and reduced general health.[18]
In children, excessive vitamin A intake can cause seborrhoeic dermatitis.[19] Lack of biotin,[18] pyridoxine (vitamin B6)[18][20] and riboflavin (vitamin B2)[18] may also be a cause.
Those with immunodeficiency (especially infection with HIV) and with neurological disorders such as Parkinson's disease (for which the condition is an autonomic sign) and stroke are particularly prone to it.[21]
Prevention
Daily use of an over-the-counter or prescription anti-fungal shampoo containing ketoconazole or zinc pyrithione may help in those with recurrent episodes of the disease.
Both natural and artificial UV radiation curbs the growth of Malassezia yeast.[22]
Management
Medications
A number of medications are able to control seborrheic dermatitis including: certain antifungals, topical corticosteroids, and keratolytics such as topical urea, as well as antiandrogens and antihistamines.[1]
Antifungals
The topical antifungal medications ketoconazole and ciclopirox have the best evidence.[3] It is unclear if other antifungals are equally effective as this has not been studied.[3]
Antiandrogens
Seborrhea is recognized as an androgen-sensitive condition – that is, it is caused or aggravated by androgen sex hormones such as testosterone and dihydrotestosterone – and is a common symptom of hyperandrogenism (e.g., that seen in polycystic ovary syndrome).[23][24] In addition, seborrhea, as well as acne, are commonly associated with puberty due to the steep increase of androgen levels at that time.[25]
In accordance with the involvement of androgens in seborrhea, antiandrogens, such as cyproterone acetate,[26] spironolactone,[27] and flutamide,[28][29] are highly effective in alleviating the condition.[23][30] As such, they are used in the treatment of seborrhea,[23][30] particularly severe cases.[31] While beneficial in seborrhea, effectiveness may vary with different antiandrogens; for instance, spironolactone (which is regarded as a relatively weak antiandrogen) has been found to produce a 50% improvement after three months of treatment, whereas flutamide has been found to result in an 80% improvement within three months.[23][29] Cyproterone acetate is similarly more potent and effective than spironolactone, and results in considerable improvement or disappearance of acne and seborrhea in 90% of patients within three months.[32]
Systemic antiandrogen therapy should only be used to treat seborrhea in women, as these drugs can result in feminization (e.g., gynecomastia), sexual dysfunction, and infertility in males.[33][34] In addition, antiandrogens theoretically have the potential to feminize male fetuses in pregnant women, and for this reason, should always be combined with effective contraception in sexually active women who can or may become pregnant.[32]
Antihistamines
Antihistamines are used primarily to reduce itching, if present. However, research studies suggest that some antihistamines have anti-inflammatory properties.[35]
Others
- Coal tar can be very effective, but, although no significant increased risk of cancer in human treatment with coal tar shampoos has been found,[36] caution is advised since coal tar is carcinogenic in animals, and heavy human occupational exposures do increase cancer risks.
- Pimecrolimus topical cream immunosuppressant[37]
- Isotretinoin — As a last resort in refractory disease, sebosuppressive agent isotretinoin may be used to reduce sebaceous gland activity. However, isotretinoin has potentially serious side effects and few patients with seborrhea are appropriate candidates for therapy.
Phototherapy
Some recommend photodynamic therapy using UV-A and UV-B laser or red and blue LED light to inhibit the growth of Malassezia fungus and reduce seborrhoeic inflammation.[38][39][40]
Epidemiology
Seborrhea affects 1 to 5% of the general population.[1][41][42] It is slightly more common in men, but affected women tend to have more severe symptoms.[42] The condition usually recurs throughout a person's lifetime.[43] Seborrhea can occur in any age group[43] but usually starts at puberty and peaks in incidence at around 40 years of age.[44] It can reportedly affect as many as 31% of older people.[42] Severity is worse in dry climates.[43]
See also
References
- 1 2 3 Dessinioti, C.; Katsambas, A. (2013). "Seborrheic dermatitis: etiology, risk factors, and treatments: facts and controversies.". Clin Dermatol. 31 (4): 343–51. doi:10.1016/j.clindermatol.2013.01.001. PMID 23806151.
- ↑ "Seborrhoeic dermatitis and dandruff". www.dermnetnz.org. Retrieved 11 June 2016.
- 1 2 3 4 Okokon, EO; Verbeek, JH; Ruotsalainen, JH; Ojo, OA; Bakhoya, VN (28 April 2015). "Topical antifungals for seborrhoeic dermatitis.". The Cochrane database of systematic reviews. 4: CD008138. doi:10.1002/14651858.CD008138.pub3. PMID 25933684.
- ↑ "Dermatitis Seborrheic Treatment". Retrieved June 11, 2010.
- ↑ "Seborrheic Dermatitis". Retrieved June 11, 2010.
- 1 2 "Dermatitis". Retrieved June 11, 2010.
- ↑ "What is Seborrheic Dermatitis?". Retrieved June 11, 2010.
- ↑ "Symptoms". Retrieved June 11, 2010.
- ↑ Dessinioti, C; Katsambas, A (Jul–Aug 2013). "Seborrheic dermatitis: etiology, risk factors, and treatments: facts and controversies.". Clinics in dermatology. 31 (4): 343–51. doi:10.1016/j.clindermatol.2013.01.001. PMID 23806151.
- ↑ Zieve, David. "Seborrheic Dermatits". A.D.A.M., Inc.
- ↑ Hay, R.J.; Graham-Brown, R.A.C. (1997). "Dandruff and seborrhoeic dermatitis: causes and management". Clinical and Experimental Dermatology. 22 (1): 3–6. doi:10.1046/j.1365-2230.1997.d01-231.x. PMID 9330043.
- ↑ Nowicki R (January 2006). "[Modern management of dandruff]". Polski Merkuriusz Lekarski (in Polish). 20 (115): 121–4. PMID 16617752.
- ↑ Parry, ME; Sharpe, GR (1998). "Seborrhoeic dermatitis is not caused by an altered immune response to Malassezia yeast". British Journal of Dermatology. 139 (2): 254–63. doi:10.1046/j.1365-2133.1998.02362.x. PMID 9767239.
- ↑ "Treatment of Seborrheic Dermatitis". Retrieved September 10, 2010.
- ↑ "P&G Beauty & Grooming | Role of Lipid Metabolism in Seborrheic Dermatitis (Dandruff)". Pgbeautygroomingscience.com. Retrieved 2013-01-26.
- ↑ Johnson, Betty Anne; Nunley, Julia R. (May 2000). "Treatment of seborrheic dermatitis". American Family Physician. 61 (9): 2703–10, 2713–4. PMID 10821151.
- ↑ Janniger CK, Schwartz RA (July 1995). "Seborrheic dermatitis". American Family Physician. 52 (1): 149–55, 159–60. PMID 7604759.
- 1 2 3 4 Schwartz, Robert A.; Janusz, Christopher A.; Janniger, Camila K. (July 2006). "Seborrheic dermatitis: an overview". American Family Physician. 74 (1): 125–30. PMID 16848386.
- ↑ MedlinePlus Encyclopedia Hypervitaminosis A
- ↑ Nutritional Neuropathy at eMedicine
- ↑ "Seborrhoeic dermatitis and dandruff (seborrheic eczema). DermNet NZ". . DermNet NZ. 2012-03-20. Retrieved 2012-06-10.
- ↑ Wikler, JR.; Janssen N.; Bruynzeel DP.; Nieboer C. (1990). "The effect of UV-light on pityrosporum yeasts: ultrastructural changes and inhibition of growth". Acta dermato-venereologica. Stockholm. 70 (1): 69–71. PMID 1967880.
- 1 2 3 4 Singh, Shankar; Gauthier, Sylvain; Labrie, Fernand (2000). "Androgen Receptor Antagonists (Antiandrogens) Structure-Activity Relationships". Current Medicinal Chemistry. 7 (2): 211–247. doi:10.2174/0929867003375371. ISSN 0929-8673.
- ↑ Zouboulis, Christos C.; Degitz, Klaus (2004). "Androgen action on human skin – from basic research to clinical significance". Experimental Dermatology. 13 (s4): 5–10. doi:10.1111/j.1600-0625.2004.00255.x. ISSN 0906-6705.
- ↑ De Groot LJ, Beck-Peccoz P, Chrousos G, Dungan K, Grossman A, Hershman JM, Koch C, McLachlan R, New M, Rebar R, Singer F, Vinik A, Weickert MO, Handelsman DJ. PMID 25905231. Missing or empty
|title=(help) - ↑ Kenneth L. Becker (2001). Principles and Practice of Endocrinology and Metabolism. Lippincott Williams & Wilkins. pp. 1004–. ISBN 978-0-7817-1750-2.
- ↑ G. Plewig; A.M. Kligman (6 December 2012). ACNE and ROSACEA. Springer Science & Business Media. pp. 66,685,687. ISBN 978-3-642-59715-2.
- ↑ NADIR R. FARID; Evanthia Diamanti-Kandarakis (27 February 2009). Diagnosis and Management of Polycystic Ovary Syndrome. Springer Science & Business Media. pp. 240–. ISBN 978-0-387-09718-3.
- 1 2 Bentham Science Publishers (September 1999). Current Pharmaceutical Design. Bentham Science Publishers. pp. 717–.
- 1 2 Mutschler; Hartmut Derendorf (1995). Drug Actions: Basic Principles and Theraputic Aspects. CRC Press. pp. 304–. ISBN 978-0-8493-7774-7.
- ↑ Joseph T. DiPiro; Robert L. Talbert; Gary C. Yee; Gary R. Matzke, Barbara G. Wells, L. Michael Posey (6 July 2008). Pharmacotherapy: A Pathophysiologic Approach. McGraw Hill Professional. p. 1598. ISBN 978-0-07-164325-2. Cite uses deprecated parameter
|coauthors=(help) - 1 2 A. Hughes; S. H. Hasan; G. W. Oertel; H. E. Voss, F. Bahner, F. Neumann, H. Steinbeck, K.-J. Gräf, J. Brotherton, H. J. Horn, R. K. Wagner (27 November 2013). Androgens II and Antiandrogens / Androgene II und Antiandrogene. Springer Science & Business Media. pp. 351, 516. ISBN 978-3-642-80859-3. Cite uses deprecated parameter
|coauthors=(help) - ↑ Larry E. Millikan (19 April 2016). Drug Therapy in Dermatology. CRC Press. pp. 295–. ISBN 978-0-203-90831-0.
- ↑ Sara Brenner (13 December 2013). The Clinical Nanomedicine Handbook. CRC Press. pp. 97–. ISBN 978-1-4398-3478-7.
- ↑ Grob, JJ; Castelain, M.; Richard, MA; Bonniol, JP; Beraud, V.; Adhoute, H.; Guillou, N.; Bonerandi, JJ (1998). "Antiinflammatory properties of cetirizine in a human contact dermatitis model. Clinical evaluation of patch tests is not hampered by antihistamines.". Acta Dermato-Venereologica. 78 (3): 194–7. doi:10.1080/000155598441512.
- ↑ Roelofzen JH, Aben KK, Oldenhof UT, et al. (April 2010). "No increased risk of cancer after coal tar treatment in patients with psoriasis or eczema". J. Invest. Dermatol. 130 (4): 953–61. doi:10.1038/jid.2009.389. PMID 20016499.
- ↑ Firooz, A.; Solhpour, A; Gorouhi, F; Daneshpazhooh, M; Balighi, K; Farsinejad, K; Rashighi-Firoozabadi, M; Dowlati, Y (2006). "Pimecrolimus Cream, 1%, vs Hydrocortisone Acetate Cream, 1%, in the Treatment of Facial Seborrheic Dermatitis: A Randomized, Investigator-Blind, Clinical Trial". Archives of Dermatology. 142 (8): 1066–1067. doi:10.1001/archderm.142.8.1066. PMID 16924062.
- ↑ Wikler JR, Janssen N, Bruynzeel DP, Nieboer C (1990). "The effect of UV-light on pityrosporum yeasts: ultrastructural changes and inhibition of growth". Acta Dermato-venereologica. 70 (1): 69–71. PMID 1967880.
- ↑ Calzavara-Pinton PG, Venturini M, Sala R (2005). "A comprehensive overview of photodynamic therapy in the treatment of superficial fungal infections of the skin". Photochem Photobiol. 78 (1): 1–6. doi:10.1016/j.jphotobiol.2004.06.006. PMID 15629243.
- ↑ "Antibacterial photodynamic therapy in dermatology – Photochemical & Photobiological Sciences (RSC Publishing)". rsc.org.
- ↑ Mark A. Goldstein; Myrna Chandler Goldstein; Larry P. Credit (17 March 2009). Your Best Medicine: From Conventional and Complementary Medicine--Expert-Endorsed Therapeutic Solutions to Relieve Symptoms and Speed Healing. Rodale. pp. 462–. ISBN 978-1-60529-656-2.
- 1 2 3 Miranda A. Farage; Kenneth W. Miller; Howard I. Maibach (2 December 2009). Textbook of Aging Skin. Springer Science & Business Media. pp. 534–. ISBN 978-3-540-89655-5.
- 1 2 3 Jeanette Jacknin (2001). Smart Medicine for Your Skin: A Comprehensive Guide to Understanding Conventional and Alternative Therapies to Heal Common Skin Problems. Penguin. pp. 271–. ISBN 978-1-58333-098-2.
- ↑ Ooi ET, Tidman MJ (2014). "Improving the management of seborrhoeic dermatitis". Practitioner. 258 (1768): 23–6, 3. PMID 24689165.
External links
| Wikimedia Commons has media related to Seborrhoeic dermatitis. |