Patch test
| Patch test | |
|---|---|
| Intervention | |
 Patch test | |
| MeSH | D010328 |
A patch test is a method used to determine whether a specific substance causes allergic inflammation of a patient's skin. Any individual suspected of having allergic contact dermatitis or atopic dermatitis needs patch testing.
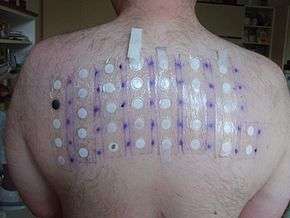
Patch testing helps identify which substances may be causing a delayed-type allergic reaction in a patient, and may identify allergens not identified by blood testing or skin prick testing. It is intended to produce a local allergic reaction on a small area of the patient's back, where the diluted chemicals were planted. The chemicals included in the patch test kit are the offenders in approximately 85–90 percent of contact allergic eczema, and include chemicals present in metals (e.g., nickel), rubber, leather, formaldehyde, lanolin, fragrance, toiletries, hair dyes, medicine, pharmaceutical items, food, drink, preservative, and other additives.
Mechanism
A patch test relies on the principle of a type IV hypersensitivity reaction.
The first step in becoming allergic is sensitization. When skin is exposed to an allergen, the antigen presenting cells (APCs) – also known as Langerhans cell or Dermal Dendritic Cell – eat up the substance (phagocytoze) and break it into smaller pieces. This is where a substance is recognized by immune cells in the skin. They then put parts of the substance onto their surface (technically holds the part of the molecule on the surface in the major histocompatibility complex type two (MHC-II). Once this is done, the APC moves down the lymphatic system to a lymph node, where it presents this part of the substance (what we now call an antigen) to a particular immune cell called a CD4+ T-cell, or T-helper cell. The T-cell, if it recognizes the substance as dangerous, expands in number and sends out more of itself to the skin, at the site of antigen exposure.
When the skin is again exposed to the antigen, the memory t-cells in the skin recognize the antigen and produce cytokines (chemical signals), which cause more T-cells to migrate from blood vessels. This starts a complex immune cascade leading to skin inflammation, itching, and the typical rash of contact dermatitis.
In general, it takes 2–4 days for a response in patch testing to develop. The patch test is just induction of a contact dermatitis in a small area.
Process
Avoid taking oral prednisone or other immunosuppressive medications for at least a week prior to testing. Steroid inhalers are OK to use. Avoid sunlight/sunburn for at least a week on the back, as this may suppress positive reactions. Antihistamines such as diphenhydramine (Benadryl) or cetirizine (Zyrtec) are permissible prior to and during testing.
Application of the patch tests will take about half an hour, though many times the overall appointment time will be longer as the provider will take an extensive history. Tiny quantities of 25 to ~150 materials (allergens) in individual square plastic or round aluminium chambers are applied to the upper back. They are kept in place with special hypoallergenic adhesive tape. The patches stay in place undisturbed for at least 48 hours. Getting the back wet during patch testing should be avoided (no shower). Vigorous exercise or stretching may disrupt the test.
At the second appointment, usually 48 hours later, the patches are removed. Sometimes additional patches are applied. The back is marked with an indelible black felt tip pen or other suitable marker to identify the test sites, and a preliminary reading is done. These marks must be visible at the third appointment, usually 24–48 hours later (72–96 hours after application). In some cases, a reading at 7 days may be requested, especially if a special metal series is tested.
Interpretation of results
The dermatologist or allergist will complete a record form at the second and third appointments (usually 48 and 72/96 hour readings). The result for each test site is recorded. One system used is as follows:


- Negative (-)
- Irritant reaction (IR)
- Equivocal / uncertain (+/-)
- Weak positive (+)
- Strong positive (++)
- Extreme reaction (+++)
Irritant reactions include miliaria (sweat rash), follicular pustules, and burn-like reactions. Uncertain reactions refer to a pink area under the test chamber. Weak positives are slightly elevated pink or red plaques, usually with mild vesiculation. Strong positives are ‘papulovesicles’ and extreme reactions have spreading redness, severe itching, and blisters or ulcers.
Relevance is determined by exposure to the positive allergen(s), and is rated as definite, probable, possible, past, or unknown. For an allergen to have definite relevance, the product the patient is exposed to must be tested and also be positive in addition to the test allergen. Probable would be used to describe a positive allergen ingredient which is in a product the patient uses (i.e., quaternium-15 listed in a moisturizing cream used on the sites of dermatitis). Interpretation of the results requires considerable experience and training. A positive patch test might not explain the present skin problem, since the test only indicates that the individual became allergic during encounters with that chemical at some point in their life. Relevance, therefore, has to be established by determining the causal relationship between the positive test and the eczema. The confirmation of relevance will occur after the patient has avoided exposure to the chemical and after he has noticed that the improvement or clearance of his dermatitis is directly related to this avoidance. This outcome usually occurs within four to six weeks after stopping the exposure to the chemical.
If all patch tests are negative, the allergic reaction is probably not due to an allergic reaction to a contactant. It is possible, however, that the patient was not tested for other chemicals that can produce allergic reactions on rare occasions. If the suspicion is high in spite of negative patch testing, further investigation might be required.
Common allergens
The top allergens from 2005–06 were: nickel sulfate (19.0%), Myroxylon pereirae (Balsam of Peru, 11.9%), fragrance mix I (11.5%), quaternium-15 (10.3%), neomycin (10.0%), bacitracin (9.2%), formaldehyde (9.0%), cobalt chloride (8.4%), methyldibromoglutaronitrile/phenoxyethanol (5.8%), p-phenylenediamine (5.0%), potassium dichromate (4.8%), carba mix (3.9%), thiuram mix (3.9%), diazolidinyl urea (3.7%), and 2-bromo-2-nitropropane-1,3-diol (3.4%).[1]
The most frequent allergen recorded in many research studies around the world is nickel. Nickel allergy is more prevalent in young women, and is especially associated with ear piercing or any nickel-containing watch, belt, zipper, or jewelry. Other common allergens are surveyed in North America by the North American Contact Dermatitis Group (NACDG).[1]
Food allergy
Dermatologists may refer a patient with a suspected food allergy for patch testing.[2] Foods identified by blood testing or skin prick testing may or may not overlap with foods identified by patch testing.[2]
Certain food additives and flavorings can cause allergic reactions around and in the mouth, around the anus and vagina as food allergens pass out of the body, or cause a widespread rash on the skin. Allergens such as nickel, Balsam of Peru, parabens, sodium benzoate, or cinnamic aldehyde may worsen or cause skin rashes.
Foods that cause urticaria (hives) or anaphylaxis (such as peanuts) cause a type I hypersensitivity reaction whereby the part of the food molecule is directly recognized by cells close to the skin, called mast cells. Mast cells have antibodies on their surface called immunoglobulin E (IgE). These act as receptors, and if they recognize the allergen, they release their contents, causing an immediate allergic reaction. Type I reactions like anaphylaxis are immediate and do not take 2 to 4 days to appear.
In a study of patients with chronic hives who were patch tested, those who were found allergic and avoided all contact with their allergen, including dietary intake, stopped having hives. Those who started eating their allergen again had recurrence of their hives.[3]
See also
References
- 1 2 Zug KA, Warshaw EM, Fowler JF Jr, Maibach HI, Belsito DL, Pratt MD, Sasseville D, Storrs FJ, Taylor JS, Mathias CG, Deleo VA, Rietschel RL, Marks J. Patch-test results of the North American Contact Dermatitis Group 2005–2006. Dermatitis. 2009 May–Jun;20(3):149-60.
- 1 2 "Food Allergy Center". Massgeneral.org. April 22, 2009. Retrieved April 6, 2014.
- ↑ Guerra L, Rogkakou A, Massacane P, Gamalero C, Compalati E, Zanella C, Scordamaglia A, Canonica WG, Passalacqua G. Role of contact sensitization in chronic urticaria. J Am Acad Dermatol 2007; 56:88–90.
External links
- Patch tests at the US National Library of Medicine Medical Subject Headings (MeSH)
- "Patch tests (contact allergy testing"), DermNet NZ