Pneumatosis intestinalis
| Pneumatosis intestinalis | |
|---|---|
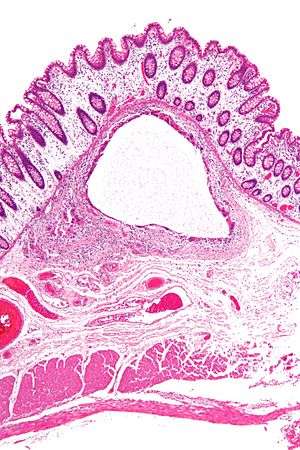 | |
| Micrograph showing large bowel wall with pneumatosis cystoides intestinalis, a generally benign subset of pneumatosis intestinalis. H&E stain. | |
| Classification and external resources | |
| ICD-10 | K63.8, R93.3 |
| ICD-9-CM | 569.89 |
| DiseasesDB | 31855 |
| eMedicine | article/371955 |
Pneumatosis intestinalis (also called intestinal pneumatosis, pneumatosis cystoides intestinalis, or pneumatosis coli) is pneumatosis of an intestine, that is, gas cysts in the bowel wall.[1] As a radiological sign it is highly suggestive for necrotizing enterocolitis. This is in contrast to gas in the intestinal lumen (which is relieved by flatulence). In newborns, pneumatosis intestinalis is considered diagnostic for necrotizing enterocolitis, and the air is produced by bacteria in the bowel wall.[2] The pathogenesis of pneumatosis intestinalis is poorly understood and is likely multifactorial. PI itself is not a disease, but rather a clinical sign. In some cases, PI is an incidental finding, whereas in others, it portends a life-threatening intra-abdominal condition.
 Pneumatosis intestinalis at computed tomography in intestinal ischemia. Lung window for better representation of the gas deposits in the intestinal walls. Coronal reconstruction.
Pneumatosis intestinalis at computed tomography in intestinal ischemia. Lung window for better representation of the gas deposits in the intestinal walls. Coronal reconstruction. Pneumatosis intestinalis in the coronal computed tomography in lung window. It can be seen next to gas entrapment in the bowel wall and gas in the stomach wall and in numerous vessels, including the portal vein into the liver.
Pneumatosis intestinalis in the coronal computed tomography in lung window. It can be seen next to gas entrapment in the bowel wall and gas in the stomach wall and in numerous vessels, including the portal vein into the liver. Pneumatosis intestinalis in computed tomography with intestinal ischemia. Lung window for better representation of the gas deposits in the intestinal walls.
Pneumatosis intestinalis in computed tomography with intestinal ischemia. Lung window for better representation of the gas deposits in the intestinal walls. Upright AP radiograph showing gas in the wall of the small bowel in the left upper quadrant indicative of pneumatosis intestinalis.
Upright AP radiograph showing gas in the wall of the small bowel in the left upper quadrant indicative of pneumatosis intestinalis. Coronal reformatted MDCT image showing extensive pneumatosis intestinalis in the left upper quadrant small bowel. The pneumatosis is more cystic and nodular in the small bowel in the midline and the right of midline. This patient had a relatively benign presentation without bowel ischemia and was treated conservatively.
Coronal reformatted MDCT image showing extensive pneumatosis intestinalis in the left upper quadrant small bowel. The pneumatosis is more cystic and nodular in the small bowel in the midline and the right of midline. This patient had a relatively benign presentation without bowel ischemia and was treated conservatively.