Benorterone
 | |
| Clinical data | |
|---|---|
| Routes of administration | Oral |
| ATC code | None |
| Identifiers | |
| |
| CAS Number | 3570-10-3 |
| PubChem (CID) | 10039776 |
| ChemSpider | 8215340 |
| UNII |
J339Q7IM54 |
| Chemical and physical data | |
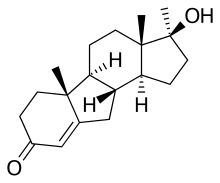
| Formula | C19H28O2 |
| Molar mass | 288.42442 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
Benorterone (INN, USAN) (developmental code names SKF-7690, FC-612), also known as 17α-methyl-B-nortestosterone, is a steroidal, pure antiandrogen that was never marketed.[1] Unlike other steroidal antiandrogens such as cyproterone acetate (CPA), it is not also a progestogen, instead acting as a selective androgen receptor antagonist similarly to non-steroidal antiandrogens such as bicalutamide.[2][3] However, although it is described as not being a progestogen, benorterone was found to produce "a highly variable decrease in plasma testosterone levels" (the reasons for this are unclear, as other pure antiandrogens such as cyproterone (not CPA) and bicalutamide do not do this and instead produce consistent increases in testosterone levels).[3]
Developed in the late 1950s and trialed in the 1960s,[1] benorterone was the first antiandrogen to be studied in humans.[4] The drug was found to be effective in the treatment of acne, seborrhea, and hirsutism in women,[3][5][6] and unlike progestogenic antiandrogens such as CPA, seldom produced side effects in women, nor affected menstruation.[3] However, in males, the drug produced gynecomastia (in 12 out of 13 young men),[7] and upon the observance of this side effect, was soon withdrawn from clinical trials.[3][4] Subsequently, CPA, which has a much reduced risk of gynecomastia by virtue of its concomitant progestogenic and antigonadotropic actions, was developed and introduced in 1973 instead.[8]
See also
- 11α-Hydroxyprogesterone
- Delanterone
- Inocoterone
- Metogest
- Rosterolone
- Topterone
- Trimethyltrienolone
- Zanoterone
References
- 1 2 J. Elks (14 November 2014). The Dictionary of Drugs: Chemical Data: Chemical Data, Structures and Bibliographies. Springer. pp. 129–. ISBN 978-1-4757-2085-3.
- ↑ Saunders, Harry L.; Holden, Kenneth; Kerwin, James F. (1964). "The anti-androgenic activity of 17α-methyl-B-nortestosterone (SK&F 7690)". Steroids. 3 (6): 687–698. doi:10.1016/0039-128X(64)90117-5. ISSN 0039-128X.
- 1 2 3 4 5 A. Hughes; S. H. Hasan; G. W. Oertel; H. E. Voss; F. Bahner; F. Neumann; H. Steinbeck; K.-J. Gräf; J. Brotherton; H. J. Horn; R. K. Wagner (27 November 2013). Androgens II and Antiandrogens / Androgene II und Antiandrogene. Springer Science & Business Media. pp. 491, 492, 517, 523. ISBN 978-3-642-80859-3.
- 1 2 Howard S. Jacobs; Royal College of Obstetricians and Gynaecologists (Great Britain) (1979). Advances in gynaecological endocrinology: proceedings of the Sixth Study Group of the Royal College of Obstetricians and Gynaecologists, 18th and 19th October, 1978. The College. p. 367. ISBN 978-0-87489-225-3.
Limited clinical experience also exists with benorterone, the first anti-androgen tried in man, and with free cyproterone. In the late sixties benorterone was reported to give promising results in 93 androgenized women but was soon withdrawn from clinical trial, mainly because of the development of gynaecomastia in the male. As a big advantage compared with CPA, it was found to be effective not only orally but also topically. Free cyproterone, on the other hand, proved to be without clinical value for reasons that cannot be discussed here. Thus we are left with CPA as the only anti-androgen that is already on the market in several countries.
- ↑ Zarate, A.; Mahesh, V. B.; Greenblatt, R. B. (1966). "Effect of an Antiandrogen, 17α-Methyl-B-nortestosterone, on Acne and Hirsutism". The Journal of Clinical Endocrinology & Metabolism. 26 (12): 1394–1398. doi:10.1210/jcem-26-12-1394. ISSN 0021-972X.
- ↑ Constantin E. Orfanos; Rudolf Happle (1990). Hair and Hair Diseases. Springer Science & Business Media. pp. 1195–. ISBN 978-3-642-74612-3.
- ↑ Sobrinho LG, Kase N, Grunt JA (1971). "Spontaneous pubertal breast growth in a castrated patient with the syndrome of testicular feminization". Yale J Biol Med. 44 (2): 225–9. PMC 2591727
 . PMID 5123057.
. PMID 5123057. - ↑ William Andrew Publishing (22 October 2013). Pharmaceutical Manufacturing Encyclopedia, 3rd Edition. Elsevier. pp. 1182–. ISBN 978-0-8155-1856-3.