Zaleplon
| |||
| Clinical data | |||
|---|---|---|---|
| Trade names | Sonata, Starnoc, Andante | ||
| AHFS/Drugs.com | Monograph | ||
| MedlinePlus | a601251 | ||
| Pregnancy category |
| ||
| Routes of administration | Oral (medical), intranasal (recreational) | ||
| ATC code | N05CF03 (WHO) | ||
| Legal status | |||
| Legal status |
| ||
| Pharmacokinetic data | |||
| Bioavailability | 30% (oral) | ||
| Metabolism | Hepatic | ||
| Biological half-life | 1–1.5 h | ||
| Excretion | Renal | ||
| Identifiers | |||
| |||
| CAS Number |
151319-34-5 | ||
| PubChem (CID) | 5719 | ||
| IUPHAR/BPS | 4345 | ||
| DrugBank |
DB00962 | ||
| ChemSpider |
5517 | ||
| UNII |
S62U433RMH | ||
| KEGG |
D00530 | ||
| ChEBI |
CHEBI:10102 | ||
| ChEMBL |
CHEMBL1521 | ||
| ECHA InfoCard | 100.126.674 | ||
| Chemical and physical data | |||
| Formula | C17H15N5O | ||
| Molar mass | 305.34 g/mol | ||
| 3D model (Jmol) | Interactive image | ||
| |||
| |||
| (verify) | |||
Zaleplon (marketed under the brand names Sonata, Starnoc, and Andante) is a sedative-hypnotic, almost entirely used for the management/treatment of insomnia. It is a nonbenzodiazepine hypnotic from the pyrazolopyrimidine class.[1]
Sonata (US) is manufactured by King Pharmaceuticals of Bristol, TN. Gedeon Richter Plc. manufactures zaleplon under the brand name Andante (RU). Starnoc has been discontinued in Canada but can be manufactured if a prescription is brought to a compounding pharmacy.[2] It is prescribed rarely in the United Kingdom, with zopiclone being the preferred Z-drug by the National Health Service (NHS).
Medical uses
Zaleplon is effective in the management/treatment of insomnia,[3] primarily characterized by difficulty falling asleep. Due to its ultrashort elimination half-life, zaleplon may not be effective in reducing premature awakenings.
It may result in an impaired ability to drive the next day, though it has proven promising when compared to other sedative/hypnotics and next-day residual sedation.[4] It may have advantages over benzodiazepines with fewer adverse effects.[5]
Neither zaleplon, nor any nonbenzodiazepine hypnotic class medication should be combined with alcohol, as both modulate GABAA receptor sites, and in a synergistic manner increase the chances of fatal respiratory depression and asphyxiation from vomiting.
Special populations
Zaleplon is not recommended for chronic use in the elderly.[6] The elderly are more sensitive to the adverse effects of zaleplon such as cognitive side effects. Zaleplon may increase the risk of injury among the elderly. It should not be used while in pregnancy or lactation, and in patients with a history of alcohol or drug abuse, psychotic illness or depression, clinicians should devote more attention.[7]
When compared with benzodiazepines, nonbenzodiazepines (including zaleplon) appear to offer few significant advantages in efficacy or tolerability among elderly individuals. Long-term use of sedative/hypnotics for insomnia has traditionally been discouraged for reasons that include concerns about such potential adverse drug effects as cognitive impairment, anterograde amnesia, daytime sedation, musculoskeletal impairment, and subsequently an increased risk of harm to oneself (e.g. falling) and to others (e.g. automotive accidents). Though, quite obviously as the body and brain age, these aforementioned phenomena are expected events, as they occur daily regardless of ingestion of a sedative/hypnotic. Thus, statistically significant and empirical evidence are arguably still absent as dramatic precautions and conclusions are drawn irrespective of the debilitating realities that accompany insomnia and the fact that these medicines do indeed provide assistance to millions of elderly individuals. It is important to distinguish between the extrapolation of potential side effects relative to the vast number of examples, wherein the sedative/hypnotic has proven therapeutically beneficial and appropriate.
In addition, some contend the efficacy and safety of long-term use of these agents remains to be enumerated, but nothing concrete suggests long-term use poses any direct harm to a person.[8]
Adverse effects
The side effects of zaleplon are similar to the side effects of benzodiazepines, although with less next-day sedation,[9] and in two studies zaleplon use was found not to cause an increase in traffic accidents, as compared to other hypnotics currently on the market.[10][11]
Available data cannot provide a reliable estimate of the incidence of dependence during treatment at recommended doses of zaleplon (typically 5–20 mg before bed). Other sedative/hypnotics have been associated with various signs and symptoms of a withdrawal syndrome, following abrupt discontinuation, ranging from mild dysphoria and insomnia to more serious cases that include abdominal and muscle cramps, vomiting, sweating, tremors, and convulsions. Following abrupt cessation, the seizure threshold is further lowered, wherein coma and death are possible outcomes if untreated.
Some evidence suggests zaleplon is not as chemically reinforcing and exhibits far fewer rebound effects when compared with other nonbenzodiazepines, or Z-drugs.[12]
Mechanism
Zaleplon, like zolpidem, zopiclone, or eszopiclone, are all specific agonists at the benzodiazepine GABAA α1 sub-receptor site. It also modulates the GABAA sub-sites, α2 and α3, to a lesser degree. It has no statistical significance as an anticonvulsant. However, as a pyrazolopyrimidine, zaleplon has served as a novel chemical platform from which new anxiolytics will hopefully arise. Much like zolpidem, as an imidazopyridine and also a full agonist at the GABAA α1 sub-receptor site, has been reviewed considerably with some novel contributions. See also: alpidem.
Pharmacology
Zaleplon selectively binds with high efficacy to the benzodiazepine site (ω1) on the α1-containing GABA-A receptors which help produce the primary therapeutic hypnotic properties. The ultrashort half-life gives zaleplon a unique advantage over other hypnotics because of its lack of next-day residual effects on driving and other performance-related skills.[13][14] Unlike nonselective benzodiazepine drugs and zopiclone, which distort the sleep pattern, zaleplon appears to induce sleep without disrupting the natural sleep architecture.[15]
A meta-analysis of randomized, controlled clinical trials which compared benzodiazepines against zaleplon or other Z-drugs such as zolpidem, zopiclone, and eszopiclone has found few clear and consistent differences between zaleplon and the benzodiazepines in terms of sleep onset latency, total sleep duration, number of awakenings, quality of sleep, adverse events, tolerance, rebound insomnia, and daytime alertness.[16]
Zaleplon has a pharmacological profile similar to benzodiazepines, characterized by an increase in slow wave deep sleep (SWDS) with rapid onset of hypnotic action. Zaleplon is a full agonist for the benzodiazepine α1 receptor located on the GABAA receptor complex in the body, with lower affinity for the α2 and α3 subsites. It selectively enhances the action of GABA similar to, but more selectively than benzodiazepines. Zaleplon, although not a benzodiazepine, maintains a very similar chemical structure nonetheless, known for inducing hypnotic effects by α1 subreceptor sites, anxiolytic, and muscle relaxant effects via α2 and α3 subsites, with negligible anticonvulsant properties (via α5 subsite), as zaleplon action is modulated at benzodiazepine receptor sites. The elimination half-life of zaleplon is about 1–1.5 hours. The absorption rate of zaleplon is rapid and the onset of therapeutic effects is typically breached within 5–15 minutes following ingestion.
Zaleplon should be understood as an ultrashort-acting sedative-hypnotic drug for the treatment of insomnia. Zaleplon increases EEG power density in the δ-frequency band and a decrease in the energy of the θ-frequency band[17][18]
Chemistry
Pure zaleplon in its solid state is a white to off-white powder with very low solubility in water, as well as low solubility in ethanol and propylene glycol. It has a partition coefficient in octanol/water that is constant (log PC = 1.23) when the pH range is between 1 and 7.
Pharmacokinetics
Zaleplon is primarily metabolised by aldehyde oxidase, and its half-life can be affected by substances which inhibit or induce aldehyde oxidase. Taken orally, zaleplon reaches full concentration in about one hour. It is extensively metabolised into 5-oxozaleplon and 5-oxodesethylzaleplon (the latter via desethylzaleplon), with less than 1% of it excreted intact in urine.
Interactions
Cimetidine, rifampicin, and thioridazine cause interactions with zaleplon.[19]
Cimetidine and grapefruit are known to increase blood plasma concentrations of benzodiazepines metabolized by the P450 CYP3A4 liver enzyme (e.g. alprazolam) by extending the time by which the drug leaves the body, effectively extending the half-life and enhancing effects to potentially toxic levels. Thus, given the similarities between zaleplon and benzodiazepines, particularly in effect, and not just chemical structure, it is reasonable to take precautions (e.g. inquire at a pharmacy) before one consumes cimetidine (or grapefruit) while also taking zaleplon.
Recreational use
Zaleplon has the potential to be a drug of abuse, and has been found to have an abuse potential similar to benzodiazepine and benzodiazepine-like hypnotics.[20] The mind- and judgment-altering effects of zaleplon are similar to those of many other benzodiazepines, but the fast-acting nature and short half-life of the chemical mean high doses set on much more quickly and last for short periods of time (usually from 45 to 60 minutes).
Some individuals use a different delivery method than prescribed, such as insufflation, to induce effects faster.[21]

A common effect of zaleplon abuse is the occurrence of (typically short-lived) hallucinations. Fewer visual and auditory hallucinations/disruptions with the use of zaleplon than with other drugs in the nonbenzodiazepine class (e.g. zolpidem and the “Ambien Walrus”). Anterograde amnesia can occur and can cause one to lose track of the amount of zaleplon already ingested, prompting one to ingest more than originally planned.[22][23] However, continuous ingestion is extremely unlikely precisely because of zaleplon's quick onset of action.
The combination of alcohol and zaleplon can result in fatal respiratory depression and asphyxiation from vomiting.
Aviation use
The FAA allows zaleplon with a 6-hour wait period and no more than twice a week.[24]
Military use
The United States Air Force uses zaleplon as one of the hypnotics approved as a "no-go pill" to help aviators and special-duty personnel sleep in support of mission readiness (with a four-hour restriction on subsequent flight operation). "Ground tests" are required prior to authorization being issued to use the medication in an operational situation.[25] (The other hypnotics used as "no-go pills" are temazepam and zolpidem, which both have longer mandatory recovery periods.[25])
Synthesis
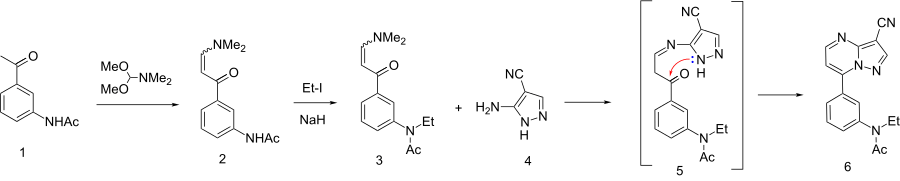
The synthesis starts with the condensation of 3-acetylacetanilide[29][30] (1) with N,N-dimethylformamide dimethyl acetal (DMFDMA)[31] to give the eneamide (2). The anilide nitrogen is then alkylated by means of sodium hydride and ethyl iodide to give 3. The first step in the condensation with 3-amino-4-cyanopyrazole can be visualized as involving an addition-elimination reaction sequence on the eneamide function to give a transient intermediate such as 5. Cyclization then leads to formation of the fused pyrimidine ring to afford zaleplon (6).
See also
References
- ↑ Elie R; Rüther E; Farr I; Emilien G; Salinas E (Aug 1999). "Sleep latency is shortened during 4 weeks of treatment with zaleplon, a novel nonbenzodiazepine hypnotic. Zaleplon Clinical Study Group". J Clin Psychiatry. 60 (8): 536–44. doi:10.4088/JCP.v60n0806. PMID 10485636.
- ↑ "Pace Pharmacy – About Our Store".
- ↑ Huedo-Medina, TB; Kirsch, I; Middlemass, J; Klonizakis, M; Siriwardena, AN (Dec 17, 2012). "Effectiveness of non-benzodiazepine hypnotics in treatment of adult insomnia: meta-analysis of data submitted to the Food and Drug Administration.". BMJ (Clinical research ed.). 345: e8343. doi:10.1136/bmj.e8343. PMC 3544552
 . PMID 23248080.
. PMID 23248080. - ↑ Verster JC, Veldhuijzen DS, Volkerts ER (August 2004). "Residual effects of sleep medication on driving ability". Sleep Med Rev. 8 (4): 309–25. doi:10.1016/j.smrv.2004.02.001. PMID 15233958.
- ↑ Barbera J, Shapiro C (2005). "Benefit-risk assessment of zaleplon in the treatment of insomnia". Drug Saf. 28 (4): 301–18. doi:10.2165/00002018-200528040-00003. PMID 15783240.
- ↑ American Geriatrics Society 2012 Beers Criteria Update Expert, Panel (April 2012). "American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults.". Journal of the American Geriatrics Society. 60 (4): 616–31. doi:10.1111/j.1532-5415.2012.03923.x. PMC 3571677. PMID 22376048.
- ↑ Antai-Otong D (August 2006). "The art of prescribing. Risks and benefits of non-benzodiazepine receptor agonists in the treatment of acute primary insomnia in older adults". Perspect Psychiatr Care. 42 (3): 196–200. doi:10.1111/j.1744-6163.2006.00070.x. PMID 16916422.
- ↑ Bain KT (June 2006). "Management of chronic insomnia in elderly persons". Am J Geriatr Pharmacother. 4 (2): 168–92. doi:10.1016/j.amjopharm.2006.06.006. PMID 16860264.
- ↑ Wagner J; Wagner ML; Hening WA (June 1998). "Beyond benzodiazepines: alternative pharmacologic agents for the treatment of insomnia". Ann Pharmacother. 32 (6): 680–91. doi:10.1345/aph.17111. PMID 9640488.
- ↑ Menzin J, Lang KM, Levy P, Levy E (January 2001). "A general model of the effects of sleep medications on the risk and cost of motor vehicle accidents and its application to France". PharmacoEconomics. 19 (1): 69–78. doi:10.2165/00019053-200119010-00005. PMID 11252547.
- ↑ Vermeeren A, Riedel WJ, van Boxtel MP, Darwish M, Paty I, Patat A (March 2002). "Differential residual effects of zaleplon and zopiclone on actual driving: a comparison with a low dose of alcohol". Sleep. 25 (2): 224–31. PMID 11905433.
- ↑ Lader MH (January 2001). "Implications of hypnotic flexibility on patterns of clinical use". Int J Clin Pract Suppl (116): 14–9. PMID 11219327.
- ↑ Patat A, Paty I, Hindmarch I (July 2001). "Pharmacodynamic profile of Zaleplon, a new non-benzodiazepine hypnotic agent". Hum Psychopharmacol. 16 (5): 369–392. doi:10.1002/hup.310. PMID 12404558.
- ↑ Rowlett JK, Spealman RD, Lelas S, Cook JM, Yin W (January 2003). "Discriminative stimulus effects of zolpidem in squirrel monkeys: role of GABA(A)/alpha1 receptors" (PDF). Psychopharmacology (Berl.). 165 (3): 209–15. doi:10.1007/s00213-002-1275-z (inactive 2015-12-08). PMID 12420154.
- ↑ Noguchi H, Kitazumi K, Mori M, Shiba T (January 2002). "Binding and neuropharmacological profile of zaleplon, a novel nonbenzodiazepine sedative/hypnotic". Eur. J. Pharmacol. 434 (1–2): 21–8. doi:10.1016/S0014-2999(01)01502-3. PMID 11755161.
- ↑ Dündar, Y; Dodd S; Strobl J; Boland A; Dickson R; Walley T. (July 2004). "Comparative efficacy of newer hypnotic drugs for the short-term management of insomnia: a systematic review and meta-analysis". Hum Psychopharmacol. 19 (5): 305–22. doi:10.1002/hup.594. PMID 15252823.
- ↑ Noguchi H; Kitazumi K; Mori M; Shiba T. (March 2004). "Electroencephalographic properties of zaleplon, a non-benzodiazepine sedative/hypnotic, in rats" (pdf). J Pharmacol Sci. 94 (3): 246–51. doi:10.1254/jphs.94.246. PMID 15037809.
- ↑ Petroski RE, Pomeroy JE, Das R, et al. (April 2006). "Indiplon is a high-affinity positive allosteric modulator with selectivity for α1 subunit-containing GABA-A benzodiazepine receptor sites." (PDF). J. Pharmacol. Exp. Ther. 317 (1): 369–77. doi:10.1124/jpet.105.096701. PMID 16399882.
- ↑ Wang JS, DeVane CL (2003). "Pharmacokinetics and drug interactions of the sedative hypnotics" (PDF). Psychopharmacol Bull. 37 (1): 10–29. doi:10.1007/BF01990373. PMID 14561946.
- ↑ "Sonata®(zaleplon)Capsules".
- ↑ Paparrigopoulos T, Tzavellas E, Karaiskos D, Liappas I (2008). "Intranasal Zaleplon Abuse". Am J Psychiatry. 165 (11): 1489–1490. doi:10.1176/appi.ajp.2008.08030452. PMID 18981079.
- ↑ Rush CR; Frey JM; Griffiths RR (Jul 1999). "Zaleplon and triazolam in humans: acute behavioral effects and abuse potential". Psychopharmacology (Berl). 145 (1): 39–51. doi:10.1007/s002130051030. PMID 10445371.
- ↑ Ator NA (2000). "Zaleplon and triazolam: drug discrimination, plasma levels, and self-administration in baboons". Drug Alcohol Depend. 61 (1): 55–68. doi:10.1016/S0376-8716(00)00123-X. PMID 11064184.
- ↑ "Medication Database – AMAS".
- 1 2 Caldwell, J. A.; Caldwell, J. L. (July 2005). "Fatigue in Military Aviation: An Overview of US Military-Approved Pharmacological Countermeasures" (pdf). Aviation, Space, and Environmental Medicine. 76 (Supplement 1): C39–C51. PMID 16018329.
- ↑ J. P. Dusza et al., U.S. Patent 4,626,538 (1986 to Am. Cyanamid).
- ↑ Anil M. Naik et al /Int.J. ChemTech Res.2010,2(1)
- ↑ http://en.cnki.com.cn/Article_en/CJFDTotal-ZYSG200205002.htm 《China Pharmacist》 2002-05 Synthesis of Zaleplon.
- ↑ Banasik, M; Komura, H; Shimoyama, M; Ueda, K (1992). "Specific inhibitors of poly(ADP-ribose) synthetase and mono(ADP-ribosyl)transferase". The Journal of biological chemistry. 267 (3): 1569–75. PMID 1530940.
- ↑ Dehmel, Florian; Weinbrenner, Steffen; Julius, Heiko; Ciossek, Thomas; Maier, Thomas; Stengel, Thomas; Fettis, Kamal; Burkhardt, Carmen; Wieland, Heike; Beckers, Thomas (2008). "Trithiocarbonates as a Novel Class of HDAC Inhibitors: SAR Studies, Isoenzyme Selectivity, and Pharmacological Profiles". Journal of Medicinal Chemistry. 51 (13): 3985. doi:10.1021/jm800093c. PMID 18558669.
- ↑ Salomon, Robert G.; Raychaudhuri, Swadesh R. (1984). "Convenient preparation of N,N-dimethylacetamide dimethyl acetal". The Journal of Organic Chemistry. 49 (19): 3659. doi:10.1021/jo00193a045.