Phencyclidine
 | |
 | |
| Clinical data | |
|---|---|
| AHFS/Drugs.com | phencyclidine |
| Addiction liability | Moderate[1] |
| Routes of administration | Injection, insufflation, smoking, oral |
| ATC code | none |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Onset of action | 2 to 60 min[2] |
| Biological half-life | 7–46 hours |
| Duration of action | 6 to 48 hours[2] |
| Identifiers | |
| |
| CAS Number |
77-10-1 |
| PubChem (CID) | 6468 |
| IUPHAR/BPS | 4282 |
| DrugBank |
DB03575 |
| ChemSpider |
6224 |
| UNII |
J1DOI7UV76 |
| KEGG |
C07575 |
| ChEBI |
CHEBI:8058 |
| ChEMBL |
CHEMBL275528 |
| ECHA InfoCard | 100.150.427 |
| Chemical and physical data | |
| Formula | C17H25N |
| Molar mass | 243.387 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
| See also: data page | |
| | |
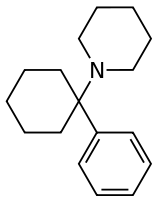
Phencyclidine (PCP), also known as angel dust and Sernyl among others,[3] is a dissociative drug. PCP was brought to market in the 1950s as an anesthetic pharmaceutical drug but was taken off the market in 1965 due to the high prevalence of dissociative hallucinogenic side effects. Moreover, the discovery of ketamine by Parke-Davis researchers was thought to represent a better-tolerated alternative for use as an anesthetic medication. Since this time a number of synthetic derivatives of PCP have been sold as dissociative drugs for recreational and non-medical use.[4]
In chemical structure, PCP is a member of the arylcyclohexylamine class, and, in pharmacology, it is a member of the family of dissociative anesthetics. PCP works primarily as an NMDA receptor antagonist, where it blocks the activity of the NMDA receptor. As an addictive drug, PCP is associated with compulsive abuse.[1][4][5][6]
As a recreational drug, PCP may be ingested orally, smoked, insufflated or injected.[7]
Recreational uses

PCP began to emerge as a recreational drug in major cities in the United States in 1967.[8]:46 In 1978, People magazine and Mike Wallace of 60 Minutes called PCP the country's "number one" drug problem. Although recreational use of the drug had always been relatively low, it began declining significantly in the 1980s. In surveys, the number of high school students admitting to trying PCP at least once fell from 13% in 1979 to less than 3% in 1990.[8]:46–49
PCP comes in both powder and liquid forms (PCP base is dissolved most often in ether), but typically it is sprayed onto leafy material such as cannabis, mint, oregano, tobacco, parsley, or ginger leaves, then smoked.
PCP is a Schedule II substance in the United States and its ACSCN is 7471.[9] Its manufacturing quota for 2014 was 19 grams.[10]
It is a Schedule I drug by the Controlled Drugs and Substances act in Canada, a List I drug of the Opium Law in the Netherlands, and a Class A substance in the United Kingdom.[11]
Methods of administration
- PCP can be ingested through smoking: tobacco or cannabis cigarettes can be dipped in a solution of PCP.
- PCP hydrochloride can be insufflated, depending upon the purity.
- The free base is quite hydrophobic and may be absorbed through skin and mucus membranes (often inadvertently).
Effects
Behavioral effects can vary by dosage. Low doses produce a numbness in the extremities and intoxication, characterized by staggering, unsteady gait, slurred speech, bloodshot eyes, and loss of balance. Moderate doses (5–10 mg intranasal, or 0.01–0.02 mg/kg intramuscular or intravenous) will produce analgesia and anesthesia. High doses may lead to convulsions.[12] Users frequently do not know how much of the drug they are taking due to the tendency of the drug to be produced illegally in uncontrolled conditions.[13]
Psychological effects include severe changes in body image, loss of ego boundaries, paranoia, and depersonalization. Hallucinations, euphoria, and suicidal impulses are also reported, as well as occasional aggressive behavior.[8]:48–49[12] Like many other drugs, phencyclidine has been known to alter mood states in an unpredictable fashion, causing some individuals to become detached, and others to become animated. PCP may induce feelings of strength, power, and invulnerability as well as a numbing effect on the mind.[7]
Studies by the Drug Abuse Warning Network in the 1970s show that media reports of PCP-induced violence are greatly exaggerated and that incidents of violence are unusual and often limited to individuals with reputations for aggression regardless of drug use.[8]:48 Although uncommon, events of PCP-intoxicated individuals acting in an unpredictable fashion, possibly driven by their delusions or hallucinations, have been publicized. One example is the case of Big Lurch, a former rapper with a history of violent crime, who was convicted of murdering and cannibalizing his roommate while under the influence of PCP.[14] Other commonly cited types of incidents include inflicting property damage and self-mutilation of various types, such as pulling one's own teeth.[8]:48[14] These effects were not noted in its medicinal use in the 1950s and 1960s, however, and reports of physical violence on phencyclidine have often been shown to be unfounded.[15][16]
Recreational doses of the drug also occasionally appear to induce a psychotic state that resembles a schizophrenic episode, sometimes lasting for months at a time.[17] Users generally report feeling detached from reality.[18]
Symptoms are summarized by the mnemonic device RED DANES: rage, erythema (redness of skin), dilated pupils, delusions, amnesia, nystagmus (oscillation of the eyeball when moving laterally), excitation, and skin dryness.[19]
Addiction
PCP is self-administered and induces nucleus accumbens ΔFosB expression in D1-type medium spiny neurons in animals;[1][20] it has also been shown to produce addiction in humans.[1] PCP's rewarding and reinforcing effects are at least partly mediated by blocking the NMDA receptors in the glutamatergic inputs to D1-type medium spiny neurons in the nucleus accumbens.[1]
Management of intoxication
Management of phencyclidine intoxication mostly consists of supportive care – controlling breathing, circulation, and body temperature – and, in the early stages, treating psychiatric symptoms.[21][22][23] Benzodiazepines, such as lorazepam, are the drugs of choice to control agitation and seizures (when present). Typical antipsychotics such as phenothiazines and haloperidol have been used to control psychotic symptoms, but may produce many undesirable side effects – such as dystonia – and their use is therefore no longer preferred; phenothiazines are particularly risky, as they may lower the seizure threshold, worsen hyperthermia, and boost the anticholinergic effects of PCP.[21][22] If an antipsychotic is given, intramuscular haloperidol has been recommended.[23][24][25]
Forced acid diuresis (with ammonium chloride or, more safely, ascorbic acid) may increase clearance of PCP from the body, and was somewhat controversially recommended in the past as a decontamination measure.[21][22][23] However, it is now known that only around 10% of a dose of PCP is removed by the kidneys, which would make increased urinary clearance of little consequence; furthermore, urinary acidification is dangerous, as it may induce acidosis and worsen rhabdomyolysis (muscle breakdown), which is not an unusual manifestation of PCP toxicity.[21][22]
Biochemistry and pharmacology
Pharmacodynamics
PCP is well known for its primary action on ionotropic glutamate receptors, such as the NMDA receptor in rats and in rat brain homogenate.[26][27] As such, PCP is an NMDA receptor antagonist. The role of NMDAR antagonism in the effect of PCP, ketamine and related dissociative agents was first published by the early 1980s by David Lodge[28] and colleagues.[4] Other NMDA receptor antagonists include ketamine,[29] tiletamine,[30] dextromethorphan,[31] nitrous oxide, MK-801, and dexoxadrol.
NMDA receptors are excitatory ionotropic receptors,[32] however, studies have shown that PCP unexpectedly produces substantial cortical activation in humans[33] and rodents.[34] Research also indicates that PCP inhibits nicotinic acetylcholine (nACh) receptors among other mechanisms. Analogues of PCP exhibit varying potency at nACh receptors[35] and NMDA receptors.[36] Findings demonstrate that presynaptic nicotinic acetylcholine (nACh) and NMDA receptor interactions influence postsynaptic maturation of glutamatergic synapses and consequently impact synaptic development and plasticity in the brain.[37] These effects can lead to inhibition of excitatory glutamate activity in certain brain regions such as the hippocampus[38] and cerebellum[39] thus potentially leading to memory loss as one of the effects of prolonged use. Acute effects on the cerebellum manifest as changes in blood pressure, breathing rate, pulse rate, and loss of muscular coordination during intoxication.[40]
PCP, like ketamine, also acts as a D2 receptor partial agonist in rat brain homogenate[27] and has affinity for human cloned D2 receptors.[41] This activity may be associated with some of the other more psychotic features of PCP intoxication, which is evidenced by the successful use of D2 receptor antagonists (such as haloperidol) in the treatment of PCP psychosis.[42]
In addition to its well explored interactions with NMDA receptors, PCP has also been to shown to associate with certain dopamine reuptake carrier proteins, and thereby lead to increased levels of available dopamine.[43]
Additionally, studies on rats indicate that PCP indirectly interacts with endorphin and enkephalin receptors to produce analgesia.[44]
Pharmacokinetics
PCP is metabolized into PCHP, PPC and PCAA.
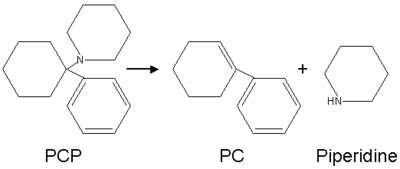
When smoked, some of the compound is broken down by heat into 1-phenylcyclohexene (PC) and piperidine.
Structural analogues
Fewer than 30 different analogues of PCP were reported as being used on the street during the 1970s and 1980s, mainly in the USA.[4] The best known of these are rolicyclidine (PCPy or 1-(1-phenylcyclohexyl)pyrrolidine); eticyclidine (PCE or N-ethyl-1-phenylcyclohexylamine); and tenocyclidine (TCP or 1-(1-(2-thienyl)cyclohexyl)piperidine).[45] Only of a few of these compounds were widely used.[4]
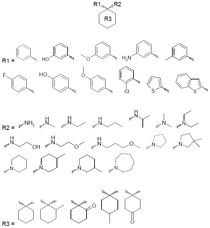
The generalized structural motif required for PCP-like activity is derived from structure-activity relationship studies of PCP derivatives, and summarized in the illustration (right). All of these derivatives are likely to share some of their psychoactive effects with PCP itself, although a range of potencies and varying mixtures of anesthetic, dissociative and stimulant effects are known, depending on the particular drug and its substituents. In some countries such as the USA, Australia, and New Zealand, all of these compounds would be considered controlled substance analogues of PCP, and are hence illegal drugs if sold for human consumption, even though many of them have never been made or tested.[46][47]
Brain effects
Some studies found that, like other NMDA receptor antagonists, phencyclidine can cause a kind of brain damage called Olney's lesions in rats.[48][49] Studies conducted on rats showed that high doses of the NMDA receptor antagonist dizocilpine caused reversible vacuoles to form in certain regions of the rats' brains. All studies of Olney's lesions have only been performed on non-human animals and may not apply to humans. One unpublished study by Frank Sharp reportedly showed no damage by the NDMA antagonist, ketamine, a similar drug, far beyond recreational doses,[50] but due to the study never having been published, its validity is controversial.
Phencyclidine has also been shown to cause schizophrenia-like changes in N-acetylaspartate and N-acetylaspartylglutamate levels in the rat brain, which are detectable both in living rats and upon necropsy examination of brain tissue.[51] It also induces symptoms in humans that mimic schizophrenia.[52]
History
It is commonly mistakenly reported that PCP was first synthesized in 1926.[53] This early synthesis, in fact, refers to the PCP intermediate PCC.[4] PCP was actually discovered by Victor Maddox, a chemist at Parke-Davis in Michigan, while investigating synthetic analgesic agents. Although unexpected, PCP was identified as potentially interesting, and as such, was submitted for pharmacological testing. The promising results of these pharmacological investigations led to the rapid development of PCP. It was approved for use as an investigational drug under the tradename Sernyl in the 1950s as an anesthetic, but because of its long half-life and adverse side effects, such as hallucinations, mania, delirium, and disorientation, it was removed from the market in 1965 and limited to veterinary use.[4][54][55]
See also
References
- 1 2 3 4 5 Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. pp. 374–375. ISBN 9780071481274.
Phencyclidine (PCP or angel dust) and ketamine (also known as special K) are structurally related drugs that are classified as dissociative anesthetics. These drugs are distinguished from other psychotomimetic agents, such as hallucinogens, by their distinct spectrum of pharmacologic effects, including their reinforcing properties and risks related to compulsive abuse ... The reinforcing properties of PCP and ketamine are mediated by the binding of these drugs to specific sites in the channel of the NMDA glutamate receptor, where they act as noncompetitive antagonists. PCP is self-administered directly into the NAc, where its reinforcing effects are believed to result from the blockade of excitatory glutamatergic input to the same medium spiny NAc neurons inhibited by opioids and dopamine
- 1 2 Riviello, Ralph J. (2010). Manual of forensic emergency medicine : a guide for clinicians. Sudbury, Mass.: Jones and Bartlett Publishers. pp. 41–42. ISBN 9780763744625.
- ↑ US Department of Justice, National Drug Intelligence Center. PCP Fast Facts
- 1 2 3 4 5 6 7 Morris H, Wallach J (2014). "From PCP to MXE: a comprehensive review of the non-medical use of dissociative drugs". Drug Testing and Analysis. 6 (7-8): 614–32. doi:10.1002/dta.1620. PMID 24678061.
- ↑ Drugs and Behavior, 4th Edition, McKim, William A., ISBN 0-13-083146-8
- ↑ Kapur, S. and P. Seeman. "NMDA receptor antagonists ketamine and PCP have direct effects on the dopamine D2 and serotonin 5-HT2receptorsimplications for models of schizophrenia(2002)
- 1 2 "NIDA InfoFacts: Hallucinogens – LSD, Peyote, Psilocybin, and PCP". DrugAbuse.gov. National Institute on Drug Abuse. Retrieved 2011-01-26.
- 1 2 3 4 5 Inciardi, James A. (1992). The War on Drugs II. Mayfield Publishing Company. ISBN 1-55934-016-9.
- ↑ US Drug Enforcement Administration March 12, 2014 Controlled Substances Page accessed June 15, 2014
- ↑ US Drug Enforcement Administration August 30, 2013. Established Aggregate Production Quotas for Schedule I and II Controlled Substances and Established Assessment of Annual Needs for the List I Chemicals Ephedrine, Pseudoephedrine, and Phenylpropanolamine for 2014 Page Accessed June 15, 2014
- ↑ "The Misuse of Drugs Act 1971 (Modification) Order 1979". www.legislation.gov.uk. Retrieved 2016-01-31.
- 1 2 Diaz, Jaime. How Drugs Influence Behavior. Englewood Cliffs: Prentice Hall, 1996.
- ↑ Chudler, Eric H. "Neuroscience for Kids – PCP". Neuroscience for Kids. Retrieved 2011-01-26.
- 1 2 Does PCP turn people into cannibals? The Straight Dope, 2005
- ↑ Brecher M, Wang BW, Wong H, Morgan JP (Dec 1988). "Phencyclidine and violence: clinical and legal issues". Journal of Clinical Psychopharmacology. 8 (6): 397–401. doi:10.1097/00004714-198812000-00003. PMID 3069880.
- ↑ Wish ED (1986). "PCP and crime: just another illicit drug?". NIDA Research Monograph. 64: 174–89. PMID 3086733.
- ↑ Luisada, PV (1978). Petersen, RC; Stillman, RC, eds. "The phencyclidine psychosis: phenomenology and treatment" (PDF). Phencyclidine (PCP) abuse: an appraisal. Rockville, Maryland: National Institute on Drug Abuse.
- ↑ Pender JW (Oct 1972). "Dissociative anesthesia". California Medicine. 117 (4): 46–7. PMC 1518731
 . PMID 18730832.
. PMID 18730832. - ↑ Giannini, A. James (1997). Drugs of Abuse (Second ed.). Los Angeles: Practice Management Information Corp. p. 126. ISBN 1-57066-053-0.
- ↑ Nestler, EJ (October 12, 2008). "Review. Transcriptional mechanisms of addiction: role of DeltaFosB". Philos. Trans. R. Soc. Lond., B, Biol. Sci. 363 (1507): 3245–3255. doi:10.1098/rstb.2008.0067. PMC 2607320. PMID 18640924."Table 1: Drugs of abuse known to induce ΔFosB in nucleus accumbens after chronic administration". republished with permission by National Center for Biotechnology Information, National Institute of Health.
- 1 2 3 4 Helman RS, Habal R (October 6, 2008). "Phencyclidine Toxicity". eMedicine. Retrieved on November 3, 2008.
- 1 2 3 4 Olmedo R (2002). "Chapter 69: Phencyclidine and ketamine". In Goldfrank LR, Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS. Goldfrank's Toxicologic Emergencies. New York: McGraw-Hill. pp. 1034–1041. ISBN 0-07-136001-8.
- 1 2 3 Milhorn HT (Apr 1991). "Diagnosis and management of phencyclidine intoxication". American Family Physician. 43 (4): 1293–302. PMID 2008817.
- ↑ Giannini AJ, Price WA (1985). "PCP: Management of acute intoxication". Medical Times. 113 (9): 43–49.
- ↑ Giannini AJ, Eighan MS, Loiselle RH, Giannini MC (Apr 1984). "Comparison of haloperidol and chlorpromazine in the treatment of phencyclidine psychosis". Journal of Clinical Pharmacology. 24 (4): 202–4. doi:10.1002/j.1552-4604.1984.tb01831.x. PMID 6725621.
- ↑ Large CH, Bison S, Sartori I, Read KD, Gozzi A, Quarta D, Antolini M, Hollands E, Gill CH, Gunthorpe MJ, Idris N, Neill JC, Alvaro GS (Jul 2011). "The efficacy of sodium channel blockers to prevent phencyclidine-induced cognitive dysfunction in the rat: potential for novel treatments for schizophrenia". The Journal of Pharmacology and Experimental Therapeutics. 338 (1): 100–13. doi:10.1124/jpet.110.178475. PMID 21487071.
- 1 2 Seeman P, Guan HC, Hirbec H (Aug 2009). "Dopamine D2High receptors stimulated by phencyclidines, lysergic acid diethylamide, salvinorin A, and modafinil". Synapse. 63 (8): 698–704. doi:10.1002/syn.20647. PMID 19391150.
- ↑ N. A. Anis, S. C. Berry, N. R. Burton & D. Lodge (1983). "The dissociative anaesthetics, ketamine and phencyclidine, selectively reduce excitation of central mammalian neurones by N-methyl-aspartate". British Journal of Pharmacology. 79 (2): 565–575. doi:10.1111/j.1476-5381.1983.tb11031.x. PMC 2044888. PMID 6317114.
- ↑ Caddy C, Giaroli G, White TP, Shergill SS, Tracy DK (Apr 2014). "Ketamine as the prototype glutamatergic antidepressant: pharmacodynamic actions, and a systematic review and meta-analysis of efficacy". Therapeutic Advances in Psychopharmacology. 4 (2): 75–99. doi:10.1177/2045125313507739. PMID 24688759.
- ↑ Klockgether T, Turski L, Schwarz M, Sontag KH, Lehmann J (Oct 1988). "Paradoxical convulsant action of a novel non-competitive N-methyl-D-aspartate (NMDA) antagonist, tiletamine". Brain Research. 461 (2): 343–8. doi:10.1016/0006-8993(88)90265-X. PMID 2846121.
- ↑ Burns JM, Boyer EW (2013). "Antitussives and substance abuse". Substance Abuse and Rehabilitation. 4: 75–82. doi:10.2147/SAR.S36761. PMC 3931656. PMID 24648790.
- ↑ Hirsch JC, Crepel F (1991). "Blockade of NMDA receptors unmasks a long-term depression in synaptic efficacy in rat prefrontal neurons in vitro". Experimental Brain Research. 85 (3): 621–4. doi:10.1007/BF00231747. PMID 1680738.
- ↑ Breier A, Malhotra AK, Pinals DA, Weisenfeld NI, Pickar D (Jun 1997). "Association of ketamine-induced psychosis with focal activation of the prefrontal cortex in healthy volunteers". The American Journal of Psychiatry. 154 (6): 805–11. doi:10.1176/ajp.154.6.805. PMID 9167508.
- ↑ Suzuki Y, Jodo E, Takeuchi S, Niwa S, Kayama Y (2002). "Acute administration of phencyclidine induces tonic activation of medial prefrontal cortex neurons in freely moving rats". Neuroscience. 114 (3): 769–79. doi:10.1016/S0306-4522(02)00298-1. PMID 12220577.
- ↑ Aguayo LG, Warnick JE, Maayani S, Glick SD, Weinstein H, Albuquerque EX (May 1982). "Site of action of phencyclidine. IV. Interaction of phencyclidine and its analogues on ionic channels of the electrically excitable membrane and nicotinic receptor: implications for behavioral effects". Molecular Pharmacology. 21 (3): 637–47. PMID 6287200.
- ↑ Zarantonello P, Bettini E, Paio A, Simoncelli C, Terreni S, Cardullo F (Apr 2011). "Novel analogues of ketamine and phencyclidine as NMDA receptor antagonists". Bioorganic & Medicinal Chemistry Letters. 21 (7): 2059–63. doi:10.1016/j.bmcl.2011.02.009. PMID 21334205.
- ↑ Lin H, Vicini S, Hsu FC, Doshi S, Takano H, Coulter DA, Lynch DR (Sep 2010). "Axonal α7 nicotinic ACh receptors modulate presynaptic NMDA receptor expression and structural plasticity of glutamatergic presynaptic boutons". Proceedings of the National Academy of Sciences of the United States of America. 107 (38): 16661–6. Bibcode:2010PNAS..10716661L. doi:10.1073/pnas.1007397107. PMC 2944730. PMID 20817852.
- ↑ Fisher JL, Dani JA (Oct 2000). "Nicotinic receptors on hippocampal cultures can increase synaptic glutamate currents while decreasing the NMDA-receptor component". Neuropharmacology. 39 (13): 2756–69. doi:10.1016/s0028-3908(00)00102-7. PMID 11044745.
- ↑ Prestori F, Bonardi C, Mapelli L, Lombardo P, Goselink R, De Stefano ME, Gandolfi D, Mapelli J, Bertrand D, Schonewille M, De Zeeuw C, D'Angelo E (2013). "Gating of long-term potentiation by nicotinic acetylcholine receptors at the cerebellum input stage". PLOS ONE. 8 (5): e64828. Bibcode:2013PLoSO...864828P. doi:10.1371/journal.pone.0064828. PMC 3669396. PMID 23741401.
- ↑ National Institute on Drug Abuse
- ↑ Seeman P, Ko F, Tallerico T (Sep 2005). "Dopamine receptor contribution to the action of PCP, LSD and ketamine psychotomimetics". Molecular Psychiatry. 10 (9): 877–83. doi:10.1038/sj.mp.4001682. PMID 15852061.
- ↑ Giannini AJ, Nageotte C, Loiselle RH, Malone DA, Price WA (1984). "Comparison of chlorpromazine, haloperidol and pimozide in the treatment of phencyclidine psychosis: DA-2 receptor specificity". Journal of Toxicology. Clinical Toxicology. 22 (6): 573–9. doi:10.3109/15563658408992586. PMID 6535849.
- ↑ Rothman RB, Reid AA, Monn JA, Jacobson AE, Rice KC (Dec 1989). "The psychotomimetic drug phencyclidine labels two high affinity binding sites in guinea pig brain: evidence for N-methyl-D-aspartate-coupled and dopamine reuptake carrier-associated phencyclidine binding sites". Molecular Pharmacology. 36 (6): 887–96. PMID 2557536.
- ↑ Castellani S, Giannini AJ, Adams PM (1982). "Effects of naloxone, metenkephalin, and morphine on phencyclidine-induced behavior in the rat". Psychopharmacology. 78 (1): 76–80. doi:10.1007/BF00470593. PMID 6815700.
- ↑ PCP synthesis and effects
- ↑ Itzhak Y, Kalir A, Weissman BA, Cohen S (May 1981). "New analgesic drugs derived from phencyclidine". Journal of Medicinal Chemistry. 24 (5): 496–9. doi:10.1021/jm00137a004. PMID 7241506.
- ↑ Chaudieu I, Vignon J, Chicheportiche M, Kamenka JM, Trouiller G, Chicheportiche R (Mar 1989). "Role of the aromatic group in the inhibition of phencyclidine binding and dopamine uptake by PCP analogs". Pharmacology, Biochemistry, and Behavior. 32 (3): 699–705. doi:10.1016/0091-3057(89)90020-8. PMID 2544905.
- ↑ Olney JW, Labruyere J, Price MT (Jun 1989). "Pathological changes induced in cerebrocortical neurons by phencyclidine and related drugs". Science. 244 (4910): 1360–2. Bibcode:1989Sci...244.1360O. doi:10.1126/science.2660263. PMID 2660263.
- ↑ Hargreaves RJ, Hill RG, Iversen LL (1994). "Neuroprotective NMDA antagonists: the controversy over their potential for adverse effects on cortical neuronal morphology". Acta Neurochirurgica. Supplementum. 60: 15–9. doi:10.1007/978-3-7091-9334-1_4. ISBN 978-3-7091-9336-5. PMID 7976530.
- ↑ Jansen, Karl. Ketamine: Dreams and Realities. MAPS, 2004. ISBN 0-9660019-7-4
- ↑ Reynolds LM, Cochran SM, Morris BJ, Pratt JA, Reynolds GP (Mar 2005). "Chronic phencyclidine administration induces schizophrenia-like changes in N-acetylaspartate and N-acetylaspartylglutamate in rat brain". Schizophrenia Research. 73 (2-3): 147–52. doi:10.1016/j.schres.2004.02.003. PMID 15653257.
- ↑ Murray JB (May 2002). "Phencyclidine (PCP): a dangerous drug, but useful in schizophrenia research". The Journal of Psychology. 136 (3): 319–27. doi:10.1080/00223980209604159. PMID 12206280.
- ↑ Development of PCP, 2006, CESAR (Center for Substance Abuse Research)
- ↑ Zukin, Stephen R; Sloboda, Zili; Javitt, Daniel C (2005). "Phencyclidine (PCP)". In Lowinson, Joyce H; Ruiz, Pedro; Millman, Robert B; et al. Substance Abuse: A Comprehensive Textbook (4th ed.). Philadelphia: Lippincott Williams & Wilkins. ISBN 0-7817-3474-6. Retrieved 2 December 2010.
- ↑ Maisto, Stephen A.; Mark Galizio; Gerard Joseph Connors (2004). Drug Use and Abuse. Thompson Wadsworth. ISBN 0-15-508517-4.
External links
| Wikimedia Commons has media related to Phencyclidine. |
- Erowid.org – PCP Information
- National Institute of Drug Abuse InfoFacts: PCP (Phencyclidine)
- Drugs and Human Performance Fact Sheets on Phencyclidine
- A site with information on PCP, Partnership for a Drug-Free America
- Phencyclidine and Ketamine: A View From the Street-1981 article on the use and effects of PCP
- ChemSub Online: Phencyclidine